
Working with PDF documents online is definitely very easy with our PDF tool. You can fill out 2009 here within minutes. To make our tool better and less complicated to utilize, we consistently work on new features, with our users' suggestions in mind. Getting underway is effortless! What you need to do is stick to these easy steps below:
Step 1: Press the "Get Form" button above. It'll open our tool so that you could begin filling out your form.
Step 2: The tool enables you to work with your PDF in a variety of ways. Transform it with personalized text, correct original content, and include a signature - all when it's needed!
To be able to fill out this document, make certain you enter the necessary details in each and every field:
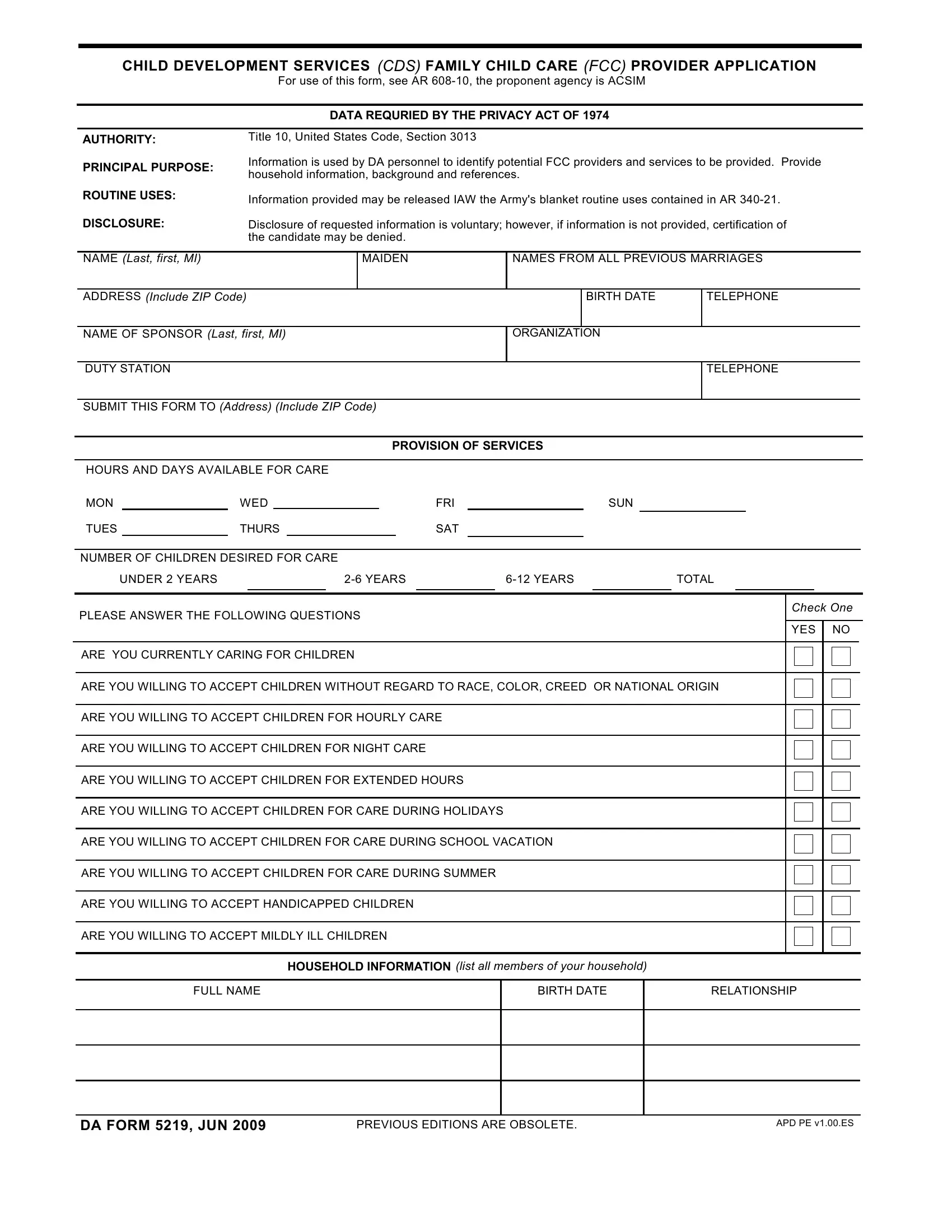
1. You will want to fill out the 2009 properly, hence take care when working with the sections containing all these blanks:
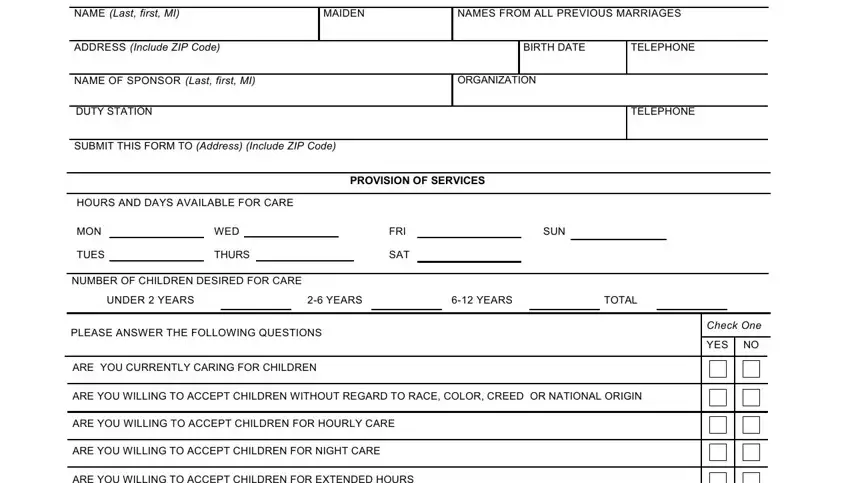
2. The third part is to fill out these fields: ARE YOU WILLING TO ACCEPT CHILDREN, ARE YOU WILLING TO ACCEPT CHILDREN, ARE YOU WILLING TO ACCEPT CHILDREN, ARE YOU WILLING TO ACCEPT CHILDREN, ARE YOU WILLING TO ACCEPT, ARE YOU WILLING TO ACCEPT MILDLY, HOUSEHOLD INFORMATION list all, FULL NAME, BIRTH DATE, RELATIONSHIP, DA FORM JUN, PREVIOUS EDITIONS ARE OBSOLETE, and APD PE vES.
3. Completing FULL NAME, BIRTH DATE, RELATIONSHIP, ARE THE MEMBERS OF YOUR HOUSEHOLD, FCC HOME SYSTEM, YES, DO YOU HAVE INDOOR HOUSEHOLD PETS, YES, WHAT IS THE LAST GRADE YOU, BACKGROUND, HAVE YOU HAD TRAINING OR OTHER, YES, HAVE YOU EVER BEEN ASKED TO RESIGN, YES, and HAVE YOU OR ANY FAMILY MEMBER OR is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. The subsequent part requires your information in the subsequent parts: ARE YOU INVOLVED IN ANY HOME, YES, PLEASE GIVE THE NAMES AND, other than relatives WHOM THE ARMY, FULL NAME, ADDRESS, TELEPHONE, REFERENCES, STATEMENT OF APPLICATION, I hereby apply to have my home, understand that in order to, pertaining to the care of children, contact me directly regarding, and Family Child Care System I certify. Make sure you give all required information to move forward.
5. To conclude your form, the last part features some additional blanks. Completing good faith, SIGNATURE, DATE, REVERSE OF DA FORM JUN, and APD PE vES will conclude everything and you're going to be done before you know it!

Always be very careful while completing DATE and APD PE vES, because this is where most people make a few mistakes.
Step 3: When you've looked once again at the details in the file's blank fields, simply click "Done" to conclude your FormsPal process. Try a 7-day free trial plan with us and get immediate access to 2009 - download or edit from your FormsPal cabinet. FormsPal guarantees safe document editor without personal information record-keeping or distributing. Feel comfortable knowing that your details are in good hands here!