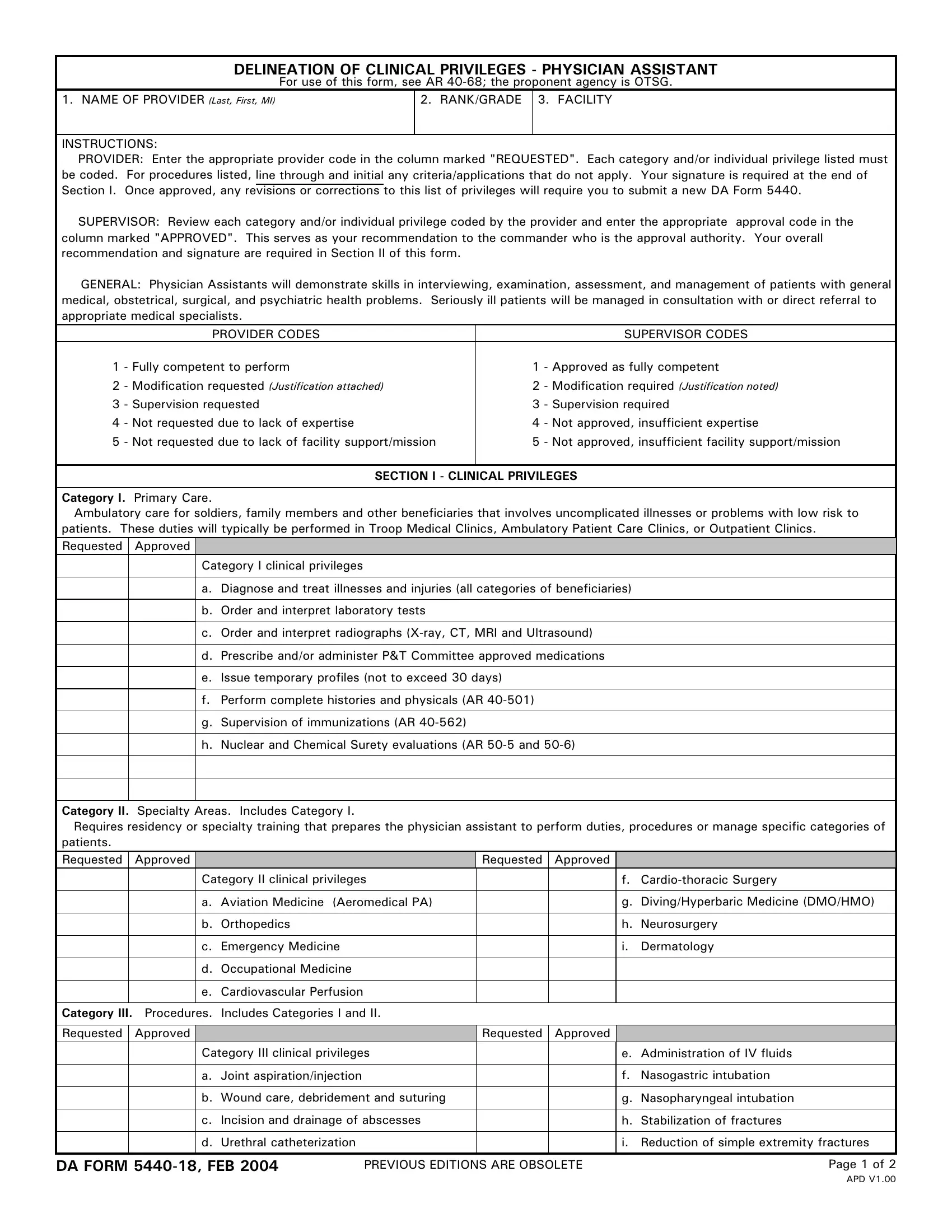
The DA Form 5440-18, titled "Delineation of Clinical Privileges - Physician Assistant," is a critical document within the U.S. Army's medical system, governed by AR 40-68, with oversight by the Office of The Surgeon General (OTSG). This form serves as a formal process for physician assistants (PAs) to request and obtain clinical privileges, endorsing their competence in various medical procedures and tasks across primary care, specialty areas, procedures, and inpatient care. The form requires PAs to specify the clinical privileges they seek, with a supervisor reviewing and offering recommendations on these requests before ultimate approval by a credentials committee or function. Categories covered range from ambulatory care for low-risk patients to specialized tasks such as first assist in major surgical cases or managing specific patient categories requiring residency or specialty training. Also, it outlines the necessity for PAs to demonstrate skills across a broad spectrum of medical tasks, including diagnostics, patient management, and specific procedural competencies. Rigorous in nature, the process ensures that only adequately trained and skilled physician assistants are granted privileges, promoting high standards of patient care and safety within military medical facilities.
| Question | Answer |
|---|---|
| Form Name | Da Form 5440 18 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | examples of physician telemedicine privilege forms, FEB, APD, radiographs |
DELINEATION OF CLINICAL PRIVILEGES - PHYSICIAN ASSISTANT
|
For use of this form, see AR |
||
1. NAME OF PROVIDER (Last, First, MI) |
|
2. RANK/GRADE |
3. FACILITY |
|
|
|
|
INSTRUCTIONS:
PROVIDER: Enter the appropriate provider code in the column marked "REQUESTED". Each category and/or individual privilege listed must be coded. For procedures listed, line through and initial any criteria/applications that do not apply. Your signature is required at the end of Section I. Once approved, any revisions or corrections to this list of privileges will require you to submit a new DA Form 5440.
SUPERVISOR: Review each category and/or individual privilege coded by the provider and enter the appropriate approval code in the column marked "APPROVED". This serves as your recommendation to the commander who is the approval authority. Your overall recommendation and signature are required in Section II of this form.
GENERAL: Physician Assistants will demonstrate skills in interviewing, examination, assessment, and management of patients with general medical, obstetrical, surgical, and psychiatric health problems. Seriously ill patients will be managed in consultation with or direct referral to appropriate medical specialists.
|
PROVIDER CODES |
|
SUPERVISOR CODES |
1 |
- Fully competent to perform |
1 |
- Approved as fully competent |
2 |
- Modification requested (Justification attached) |
2 |
- Modification required (Justification noted) |
3 |
- Supervision requested |
3 |
- Supervision required |
4 |
- Not requested due to lack of expertise |
4 |
- Not approved, insufficient expertise |
5 |
- Not requested due to lack of facility support/mission |
5 |
- Not approved, insufficient facility support/mission |
|
|
|
|
SECTION I - CLINICAL PRIVILEGES
Category I. Primary Care.
Ambulatory care for soldiers, family members and other beneficiaries that involves uncomplicated illnesses or problems with low risk to patients. These duties will typically be performed in Troop Medical Clinics, Ambulatory Patient Care Clinics, or Outpatient Clinics.
Requested Approved
Category I clinical privileges
a.Diagnose and treat illnesses and injuries (all categories of beneficiaries)
b.Order and interpret laboratory tests
c.Order and interpret radiographs
d.Prescribe and/or administer P&T Committee approved medications
e.Issue temporary profiles (not to exceed 30 days)
f.Perform complete histories and physicals (AR
g.Supervision of immunizations (AR
h.Nuclear and Chemical Surety evaluations (AR
Category II. Specialty Areas. Includes Category I. |
|
|
|
|
|||
Requires residency or specialty training that prepares the physician assistant to perform duties, procedures or manage specific categories of |
|||||||
patients. |
|
|
|
|
|
|
|
Requested |
Approved |
|
|
Requested |
Approved |
|
|
|
|
Category II clinical privileges |
|
|
f. |
||
|
|
|
|
|
|
|
|
|
|
a. Aviation Medicine |
(Aeromedical PA) |
|
|
g. |
Diving/Hyperbaric Medicine (DMO/HMO) |
|
|
|
|
|
|
|
|
|
|
b. Orthopedics |
|
|
|
h. |
Neurosurgery |
|
|
|
|
|
|
|
|
|
|
c. Emergency Medicine |
|
|
i. |
Dermatology |
|
|
|
|
|
|
|
|
|
|
|
d. Occupational Medicine |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
e. Cardiovascular Perfusion |
|
|
|
|
|
|
|
|
|
|
|
|
|
Category III. Procedures. Includes Categories I and II. |
|
|
|
|
|||
|
|
|
|
|
|
|
|
Requested |
Approved |
|
|
Requested |
Approved |
|
|
|
|
Category III clinical privileges |
|
|
e. Administration of IV fluids |
||
|
|
|
|
|
|
|
|
|
|
a. Joint aspiration/injection |
|
|
f. |
Nasogastric intubation |
|
|
|
|
|
|
|
|
|
|
|
b. Wound care, debridement and suturing |
|
|
g. |
Nasopharyngeal intubation |
|
|
|
|
|
|
|
|
|
|
|
c. Incision and drainage of abscesses |
|
|
h. |
Stabilization of fractures |
|
|
|
|
|
|
|
|
|
|
|
d. Urethral catheterization |
|
|
i. |
Reduction of simple extremity fractures |
|
|
|
|
|
|
|
|
|
DA FORM |
PREVIOUS EDITIONS ARE OBSOLETE |
Page 1 of 2 |
|||||
APD V1.00

Category III. |
(Continued) |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||
Requested |
|
Approved |
|
|
|
Requested |
Approved |
|
|
|
|
|
|
j. Administration of anesthesia |
|
|
|
k. First assist in major surgical cases |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(1) |
Digital |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(2) |
Local |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(3) |
Intercostal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Category IV. Inpatient Privileges. Includes Categories I, II and III. |
|
|
|
|
||||||
Typically requires specialty training or assignment to duties that necessitate these privileges. |
|
|||||||||
Requested |
|
Approved |
|
|
|
Requested |
Approved |
|
|
|
|
|
|
Category IV clinical privileges |
|
|
|
d. *Narrative summaries |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. *Admission of patients |
|
|
|
e. *Discharge of patients |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. *Inpatient history and physical |
|
|
|
|
|
|
|
|
|
|
examinations |
|
|
|
|
|
|
|
|
|
|
c. *Doctor's orders |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
*Requires physician review and signature within 24 hours. |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
COMMENTS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SIGNATURE OF PROVIDER |
|
DATE (YYYYMMDD) |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION II - SUPERVISOR'S RECOMMENDATION |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
Approval as requested |
Approval with Modifications (Specify below) |
|
Disapproval (Specify below) |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
COMMENTS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
DEPARTMENT/SERVICE CHIEF (Typed name and title) |
SIGNAURE |
|
|
|
DATE (YYYYMMDD) |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION III - CREDENTIALS COMMITTEE/FUNCTION RECOMMENDATION |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
Approval as requested |
Approval with Modifications (Specify below) |
|
Disapproval (Specify below) |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
COMMENTS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
COMMITTEE CHAIRPERSON (Name and rank) |
SIGNATURE |
|
|
|
DATE (YYYYMMDD) |
|||||
|
|
|
|
|
|
|
|
|
|
|
DA FORM |
|
|
|
|
|
|
Page 2 of 2 |
|||
APD V1.00