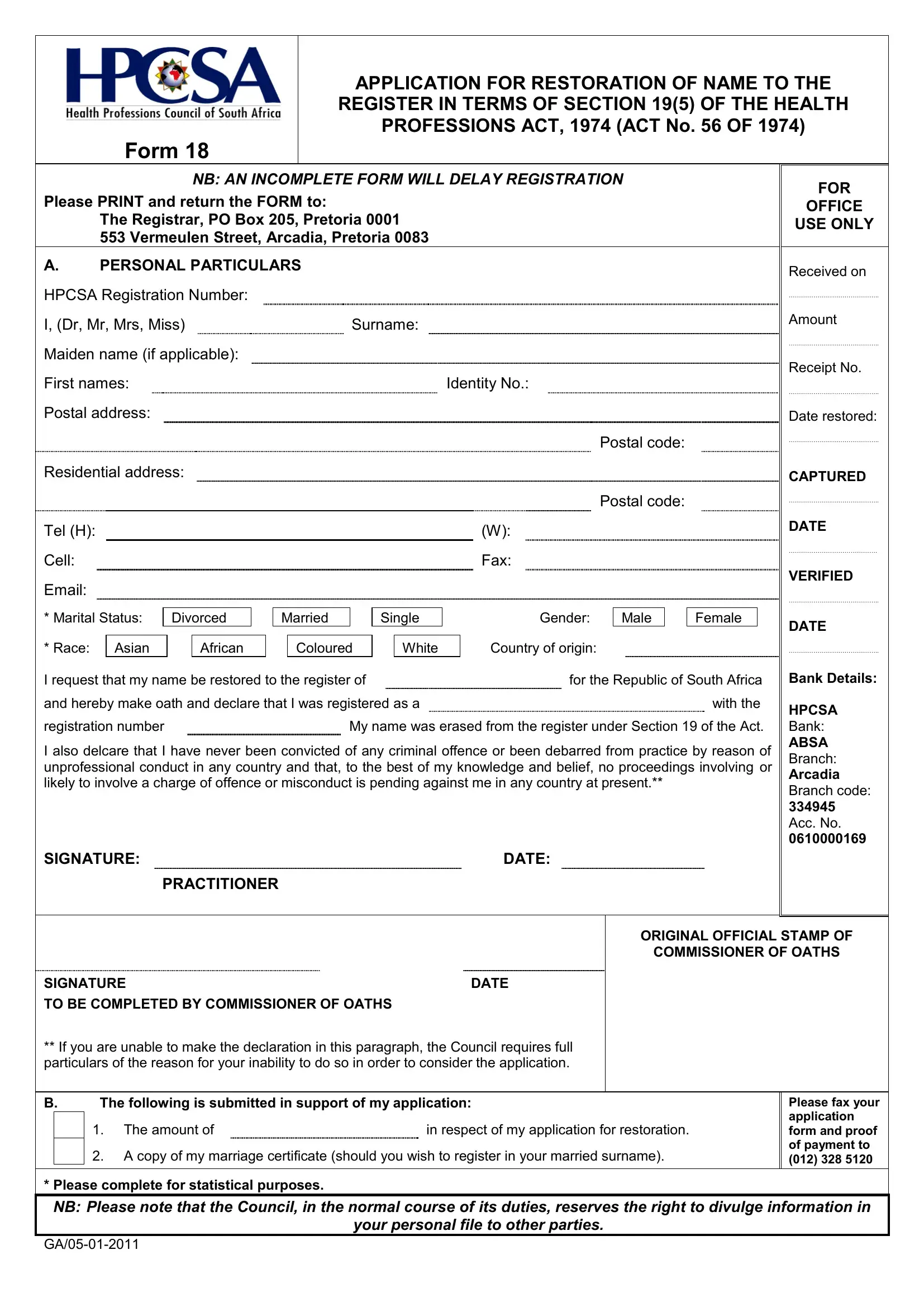
Navigating the road back to professional practice in the health sector involves many steps, one of which is the completion and submission of the HPCSA 18 form, formally known as the Application for Restoration of Name to the Register under Section 19(5) of the Health Professions Act, 1974. This pivotal document plays a crucial role for professionals seeking to reinstate their credentials and return to practice within the Republic of South Africa. Required by the Health Professions Council of South Africa, the form mandates comprehensive personal particulars, a declaration of professional conduct, and an affirmation of no criminal convictions or pending proceedings. It highlights the importance of accountability and integrity in the health professions, ensuring that those re-entering the field maintain the high standards expected by both the public and the profession. The procedure outlined in the form, including the need for supporting documents like proof of payment and, if applicable, a marriage certificate, underscores the thoroughness of the review process. Moreover, the instruction that an incomplete form will delay registration underscores the meticulousness with which the Council approaches each application, aiming to safeguard public health and trust. In essence, the HPCSA 18 form stands as a cornerstone for professionals on their path to restoration, embodying both a barrier and a gateway as they strive to resume their valuable contributions to healthcare in South Africa.
| Question | Answer |
|---|---|
| Form Name | Hpcsa Form 18 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | hpcsa login, hpcsa card download 2021, download hpcsa card, hpcsa practitioner card |