
Filling out DA Form 5440-18 correctly is essential for physician assistants who need to establish or update their clinical privileges at a U.S. Army medical treatment facility. The steps below explain each part of the process.
How to Fill Out the Form Step by Step
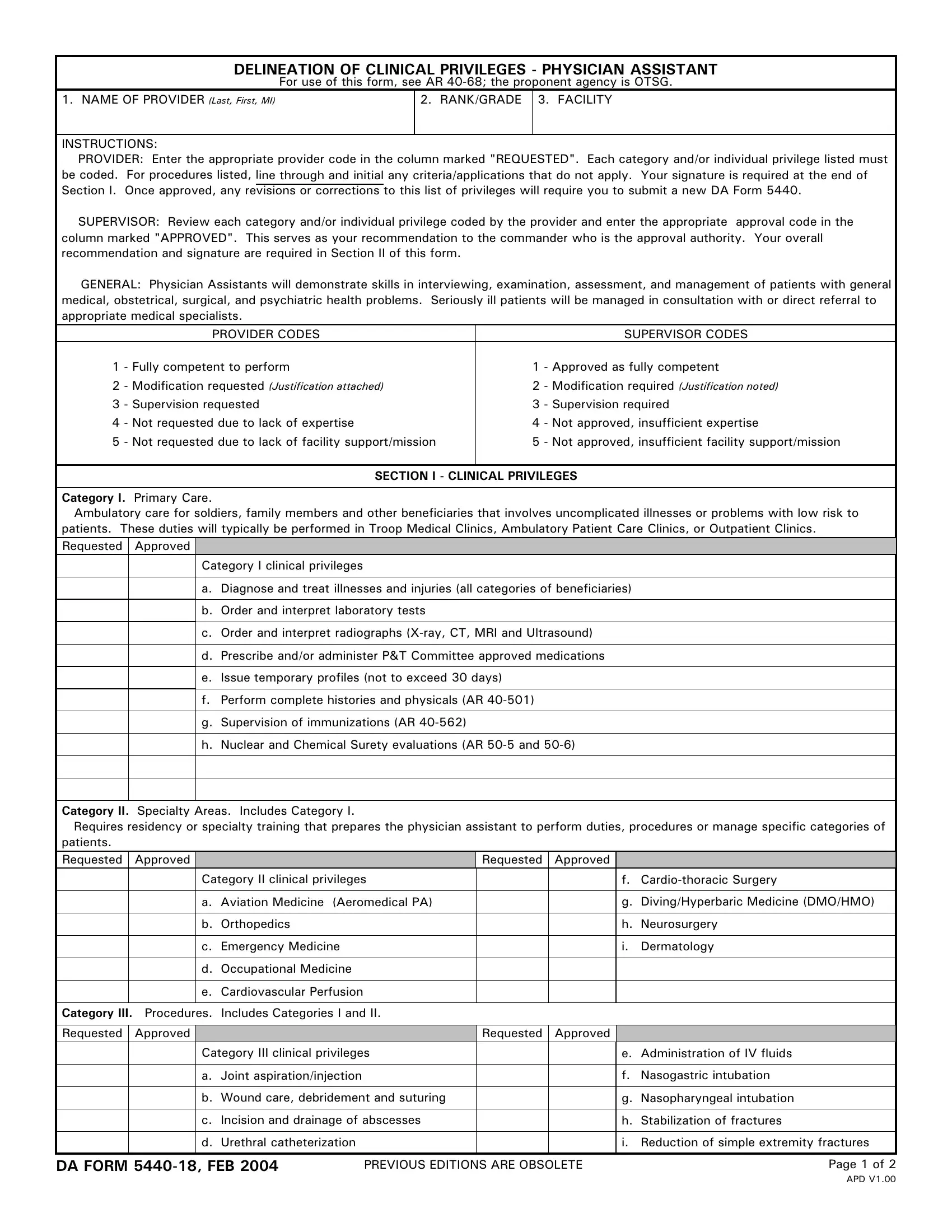
- Enter facility and unit information - At the top of the form, write the name and address of the military treatment facility (MTF), your unit designation, and the date of the request. Use the format your MTF's credentialing office requires.
- Provide your personal and professional information - Print your full name, rank, and DoD identification number as they appear in official records. Include your National Provider Identifier (NPI) number if you have one.
- List your requested clinical privileges - Review the privilege categories on the form and check each box for the privileges you are requesting. For each requested privilege, document the training source, the number of procedures you performed in the past 24 months, and any relevant certifications.
- Complete the attestation statement - Sign and date the attestation confirming that all information is accurate and that you meet the minimum competency requirements for each privilege you have selected.
- Submit for supervisor review - Present the form to your supervising physician or department head for review. Your supervisor will confirm, modify, or deny each privilege request and sign the form before it moves forward.
- Forward to the credentials office - Submit the signed form to the MTF credentials office along with any required supporting documents, such as training certificates, continuing medical education records, or case logs.
- Await the committee decision - The credentials committee reviews all materials and notifies you in writing of their decision. Approval, conditional approval with proctoring, or denial will be recorded in your credentials file.
What information must be included on the form?
The form requires your name, rank, DoD identification number, NPI, facility details, and a list of requested privileges with supporting documentation for each. Signatures from both you and your supervising physician are mandatory before submission.
How long does the credentialing process take?
Initial credentialing typically takes 30 to 60 days from the date of a complete submission. Temporary privileges may be granted during this period so that supervised patient care can continue while the full review is underway.
Can privileges be denied or revoked?
Yes. The credentials committee may deny a privilege request if the documentation does not demonstrate sufficient competency. Existing privileges may also be suspended or revoked after an adverse patient care event, a formal complaint, or a pattern of quality concerns identified through peer review. Revocation decisions are documented in the provider's credentials file.
Related Physician and Medical Forms
If you work with physician credentialing and healthcare documentation, these related forms may also be relevant to your work:
- Attending Physician Statement (Aetna) - used when documenting a patient's medical condition for insurance claim purposes
- Physician Medical Report Form - required for exchange visitor program and visa medical certifications
- Clinical Experience Form - used to document supervised clinical hours for credentialing and licensure applications
- Clinical Skills Evaluation Form - used to assess and record psychiatric clinical competencies during training