The DA Form 8001 serves a crucial role within the military healthcare system, functioning as a testament to the delicate balance between offering comprehensive care and safeguarding personal health information. Issued by the Office of The Surgeon General under the regulation AR 40-66, it outlines the boundaries of confidentiality while providing healthcare services which range from assessment and various forms of therapy to substance abuse treatment and psychiatric evaluations. Recognizing the importance of privacy, the form stipulates that personal information of patients is generally not disclosed without explicit written consent, with a few key exceptions designed to protect safety, comply with legal obligations, or meet commanding authority requirements. The exceptions include situations where there is a risk of harm to the patient or others, cases of abuse, legal proceedings, fitness for duty evaluations, care coordination, and quality care reviews ensuring standards of care are met. This form also highlights the role of healthcare providers in the military's goal of maintaining the health of service members while navigating the complexities of privacy, legal requirements, and the overall mission of the armed forces. Embedded within these processes is a dual commitment to upholding the highest standards of patient care and adhering to the regulations protecting patient information, as distilled in federal mandates like the Privacy Act, DoDI 6490.08, and the Health Insurance Portability and Accountability Act (HIPAA) of 1996.
| Question | Answer |
|---|---|
| Form Name | Da Form 8001 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 2012, 01ES, APD, da form 8001 |
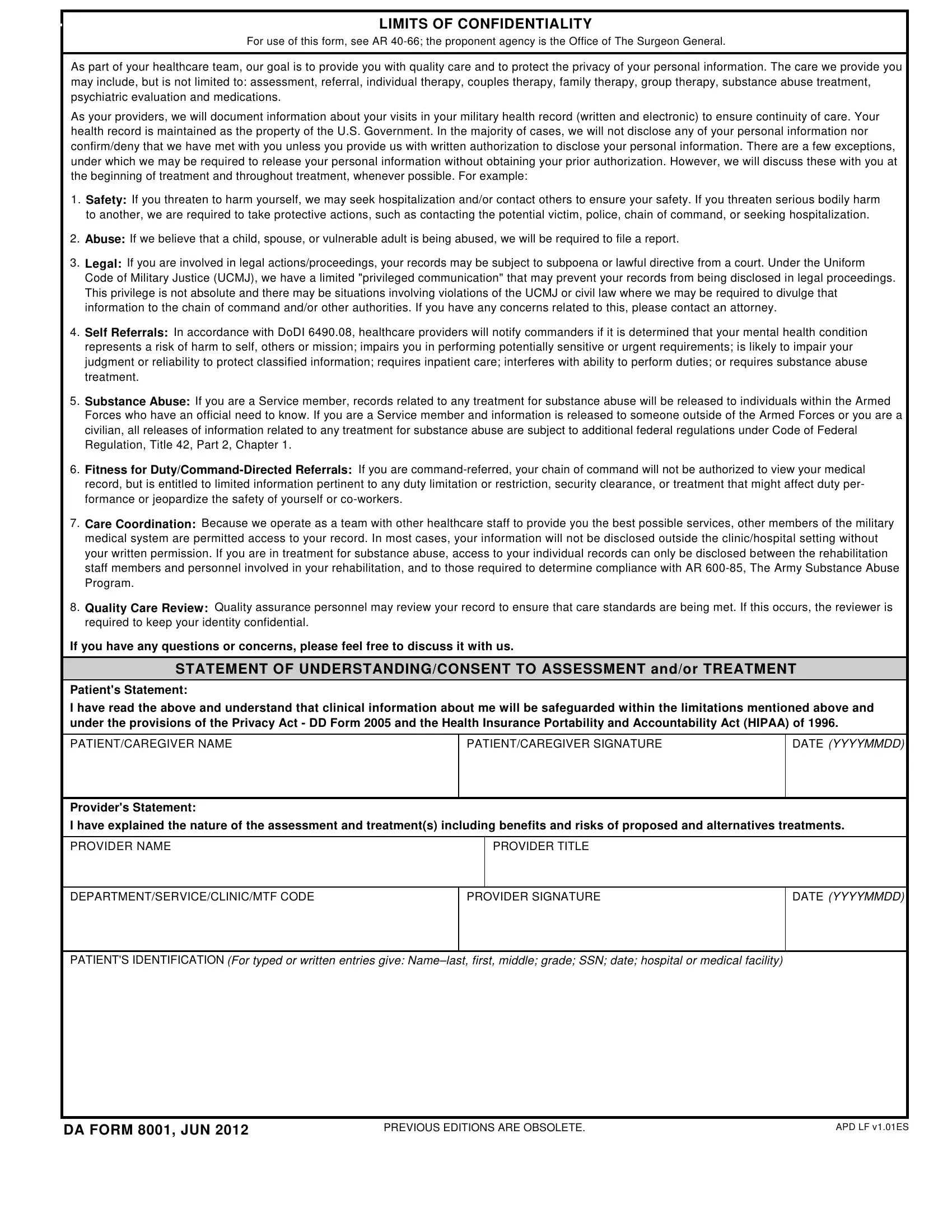
LIMITS OF CONFIDENTIALITY
For use of this form, see AR
As part of your healthcare team, our goal is to provide you with quality care and to protect the privacy of your personal information. The care we provide you may include, but is not limited to: assessment, referral, individual therapy, couples therapy, family therapy, group therapy, substance abuse treatment, psychiatric evaluation and medications.
As your providers, we will document information about your visits in your military health record (written and electronic) to ensure continuity of care. Your health record is maintained as the property of the U.S. Government. In the majority of cases, we will not disclose any of your personal information nor confirm/deny that we have met with you unless you provide us with written authorization to disclose your personal information. There are a few exceptions, under which we may be required to release your personal information without obtaining your prior authorization. However, we will discuss these with you at the beginning of treatment and throughout treatment, whenever possible. For example:
1.Safety: If you threaten to harm yourself, we may seek hospitalization and/or contact others to ensure your safety. If you threaten serious bodily harm to another, we are required to take protective actions, such as contacting the potential victim, police, chain of command, or seeking hospitalization.
2.Abuse: If we believe that a child, spouse, or vulnerable adult is being abused, we will be required to file a report.
3.Legal: If you are involved in legal actions/proceedings, your records may be subject to subpoena or lawful directive from a court. Under the Uniform Code of Military Justice (UCMJ), we have a limited "privileged communication" that may prevent your records from being disclosed in legal proceedings. This privilege is not absolute and there may be situations involving violations of the UCMJ or civil law where we may be required to divulge that information to the chain of command and/or other authorities. If you have any concerns related to this, please contact an attorney.
4.Self Referrals: In accordance with DoDI 6490.08, healthcare providers will notify commanders if it is determined that your mental health condition represents a risk of harm to self, others or mission; impairs you in performing potentially sensitive or urgent requirements; is likely to impair your judgment or reliability to protect classified information; requires inpatient care; interferes with ability to perform duties; or requires substance abuse treatment.
5.Substance Abuse: If you are a Service member, records related to any treatment for substance abuse will be released to individuals within the Armed Forces who have an official need to know. If you are a Service member and information is released to someone outside of the Armed Forces or you are a civilian, all releases of information related to any treatment for substance abuse are subject to additional federal regulations under Code of Federal Regulation, Title 42, Part 2, Chapter 1.
6.Fitness for
7.Care Coordination: Because we operate as a team with other healthcare staff to provide you the best possible services, other members of the military medical system are permitted access to your record. In most cases, your information will not be disclosed outside the clinic/hospital setting without your written permission. If you are in treatment for substance abuse, access to your individual records can only be disclosed between the rehabilitation staff members and personnel involved in your rehabilitation, and to those required to determine compliance with AR
8.Quality Care Review: Quality assurance personnel may review your record to ensure that care standards are being met. If this occurs, the reviewer is required to keep your identity confidential.
If you have any questions or concerns, please feel free to discuss it with us.
STATEMENT OF UNDERSTANDING/CONSENT TO ASSESSMENT and/or TREATMENT
Patient's Statement:
I have read the above and understand that clinical information about me will be safeguarded within the limitations mentioned above and under the provisions of the Privacy Act - DD Form 2005 and the Health Insurance Portability and Accountability Act (HIPAA) of 1996.
PATIENT/CAREGIVER NAME
PATIENT/CAREGIVER SIGNATURE
DATE (YYYYMMDD)
Provider's Statement:
I have explained the nature of the assessment and treatment(s) including benefits and risks of proposed and alternatives treatments.
PROVIDER NAME
PROVIDER TITLE
DEPARTMENT/SERVICE/CLINIC/MTF CODE
PROVIDER SIGNATURE
DATE (YYYYMMDD)
PATIENT'S IDENTIFICATION (For typed or written entries give:
DA FORM 8001, JUN 2012
PREVIOUS EDITIONS ARE OBSOLETE. |
APD LF v1.01ES |