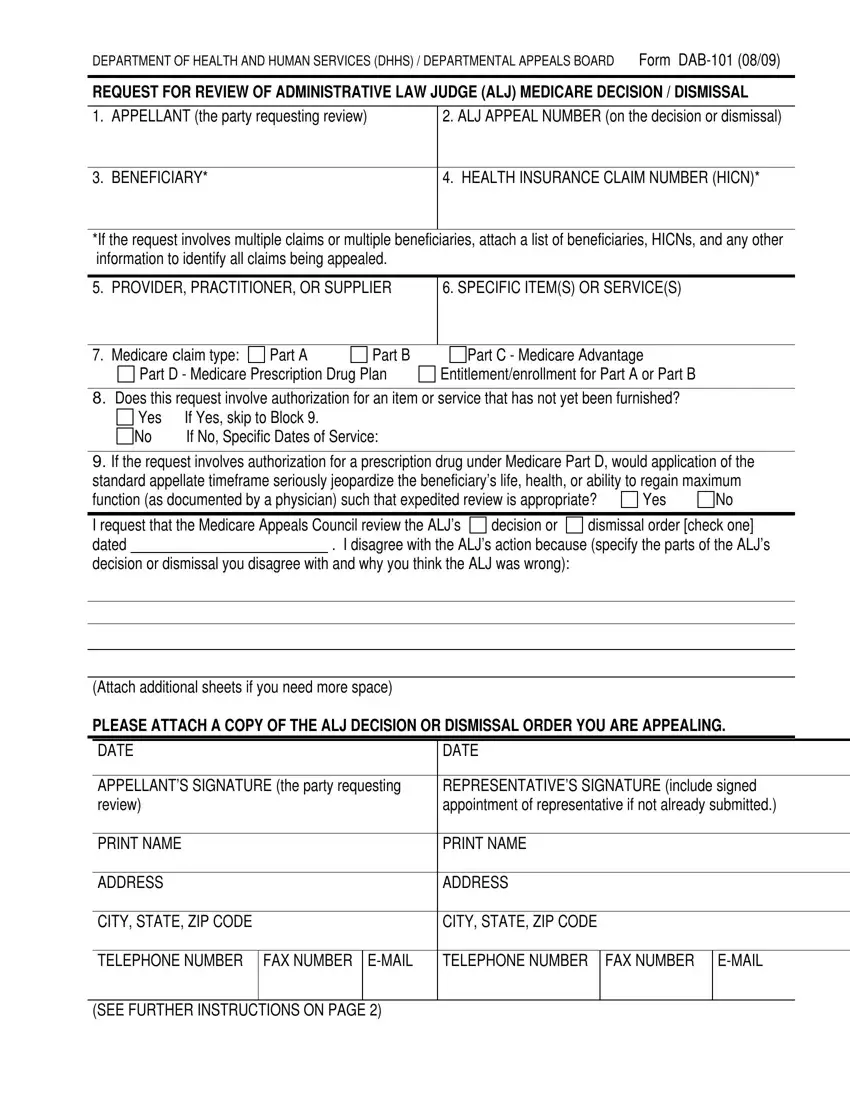
DEPARTMENT OF HEALTH AND HUMAN SERVICES (DHHS) / DEPARTMENTAL APPEALS BOARD Form DAB-101 (08/09)
REQUEST FOR REVIEW OF ADMINISTRATIVE LAW JUDGE (ALJ) MEDICARE DECISION / DISMISSAL
1. APPELLANT (the party requesting review)
2. ALJ APPEAL NUMBER (on the decision or dismissal)
4. HEALTH INSURANCE CLAIM NUMBER (HICN)*
*If the request involves multiple claims or multiple beneficiaries, attach a list of beneficiaries, HICNs, and any other information to identify all claims being appealed.
5. PROVIDER, PRACTITIONER, OR SUPPLIER
6. SPECIFIC ITEM(S) OR SERVICE(S)
7. Medicare Claim type: |
Part A |
Part B |
Part D - Medicare Prescription Drug Plan

 Part C - Medicare Advantage Entitlement/enrollment for Part A or Part B
Part C - Medicare Advantage Entitlement/enrollment for Part A or Part B
8.Does this request involve authorization for an item or service that has not yet been furnished?
Yes |
If Yes, skip to Block 9. |
No |
If No, Specific Dates of Service: |
9.If the request involves authorization for a prescription drug under Medicare Part D, would application of the standard appellate timeframe seriously jeopardize the beneficiary’s life, health, or ability to regain maximum
|
|
|
|
|
|
|
function (as documented by a physician) such that expedited review is appropriate? |
Yes |
No |
|
|
|
I request that the Medicare Appeals Council review the ALJ’s |
decision or |
dismissal order [check one] |
dated |
|
. I disagree with the ALJ’s action because (specify the parts of the ALJ’s |
decision or dismissal you disagree with and why you think the ALJ was wrong):
(Attach additional sheets if you need more space)
PLEASE ATTACH A COPY OF THE ALJ DECISION OR DISMISSAL ORDER YOU ARE APPEALING.
|
DATE |
DATE |
|
|
|
|
|
|
|
|
|
APPELLANT’S SIGNATURE (the party requesting |
REPRESENTATIVE’S SIGNATURE (include signed |
|
review) |
appointment of representative if not already submitted.) |
|
|
|
|
|
|
|
|
|
PRINT NAME |
PRINT NAME |
|
|
|
|
|
|
|
|
|
ADDRESS |
ADDRESS |
|
|
|
|
|
|
|
|
|
CITY, STATE, ZIP CODE |
CITY, STATE, ZIP CODE |
|
|
|
|
|
|
|
|
|
TELEPHONE NUMBER |
FAX NUMBER |
E-MAIL |
TELEPHONE NUMBER |
FAX NUMBER |
E-MAIL |
|
|
|
|
|
|
|
|
|
(SEE FURTHER INSTRUCTIONS ON PAGE 2) |
|
|
|
|
Form DAB-101 (08/09)
If you have additional evidence, submit it with this request for review. If you need more time, you must request an extension of time in writing now, explaining why you are unable to submit the evidence or legal argument now.
If you are a provider, supplier, or a beneficiary represented by a provider or supplier, and your case was reconsidered by a Qualified Independent Contractor (QIC), the Medicare Appeals Council will not consider new evidence related to issues the QIC has already considered unless you show that you have a
good reason for submitting it for the first time to the Medicare Appeals Council.
IMPORTANT: Include the HICN and ALJ Appeal Number on any letter or other material you submit.
This request must be received within 60 calendar days after you receive the ALJ’s decision or dismissal, unless we extend the time limit for good cause. We assume you received the decision or dismissal 5 calendar days after it was issued, unless you show you received it later. If this request will not be received within
65 calendar days from the date on the decision or dismissal order, please explain why on a separate sheet.
You must file your request for review in writing with the Medicare Appeals Council at:
Department of Health and Human Services
Departmental Appeals Board
Medicare Appeals Council, MS 6127
Cohen Building Room G-644
330 Independence Ave., S.W.
Washington, D.C. 20201
You may send the request for review by U.S. Mail, a common carrier such as FedEx, or by fax to (202) 565-0227. If you send a fax, please do not also mail a copy. You must send a copy of your appeal to the other parties and indicate that all parties, to include all beneficiaries, have been copied on the request for review. For claims involving multiple beneficiaries, you may submit a copy of the cover letters issued or a spreadsheet of the beneficiaries and addresses who received a copy of the request for review.
If you have any questions about your request for review or wish to request expedited review of a claim involving authorization of your prescription drug under Medicare Part D, you may call the Medicare Appeals Council’s staff in the Medicare Operations Division of the Departmental Appeals Board at (202) 565-0100. You may also visit our web site at www.hhs.gov/dab for additional information on how to file your request for review.
PRIVACY ACT STATEMENT
The collection of information on this form is authorized by the Social Security Act (section 205(a) of title II, section 702 of title VII, section 1155 of Title XI, and sections 1852(g)(5), 1869(b)(1), 1871, 1872, and 1876(c)(5)(B) of title XVIII, as appropriate). The information provided will be used to further document your claim. Information requested on this form is voluntary, but failure to provide all or any part of the requested information may affect the determination of your claim. Information you furnish on this form may be disclosed by the Department of Health and Human Services or the Social Security Administration to another person or governmental agency only with respect to programs under the Social Security Act and to comply with Federal laws requiring the disclosure of information or the exchange of information between the Department of Health and Human Services, the Social Security Administration, or other agencies.