
 No
No
Having the goal of making it as quick to use as possible, we established this PDF editor. The process of filling the form 3647 pdf will be trouble-free if you comply with the following steps.
Step 1: First, choose the orange "Get form now" button.
Step 2: So you will be on the document edit page. It's possible to add, modify, highlight, check, cross, add or erase fields or phrases.
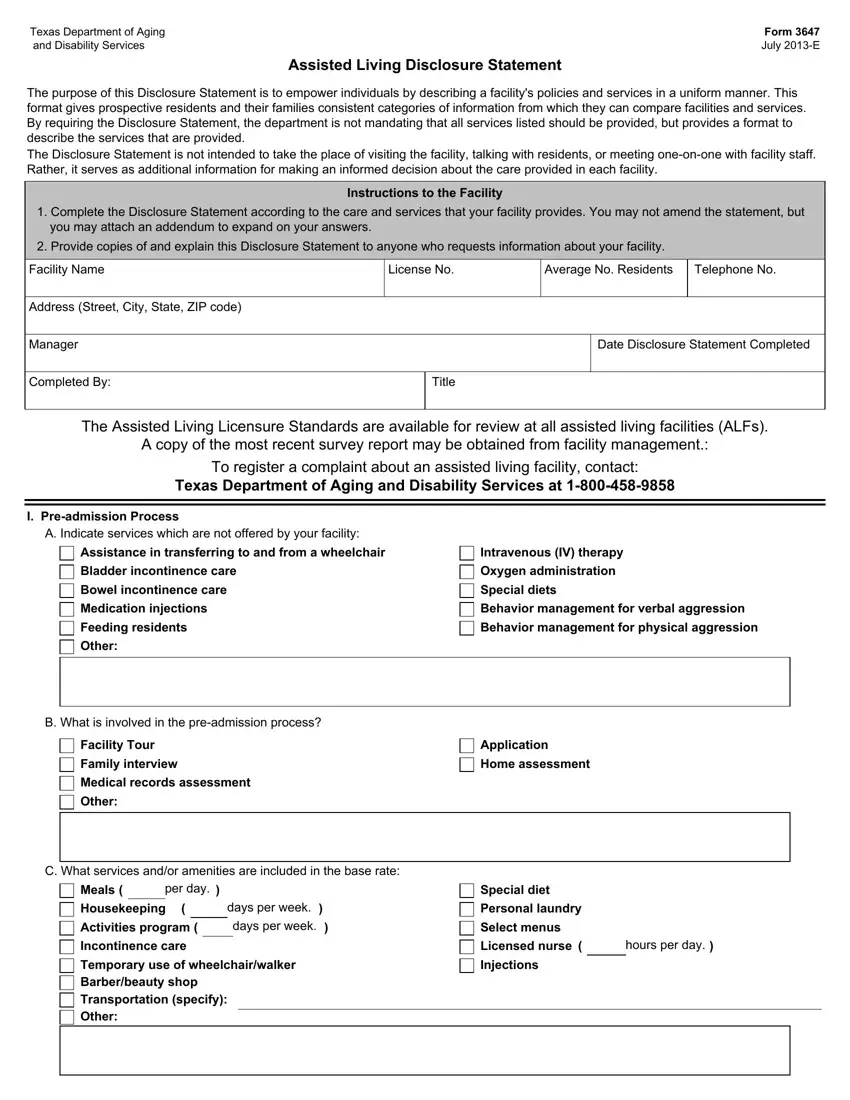
The PDF file you decide to fill out will include the next parts:
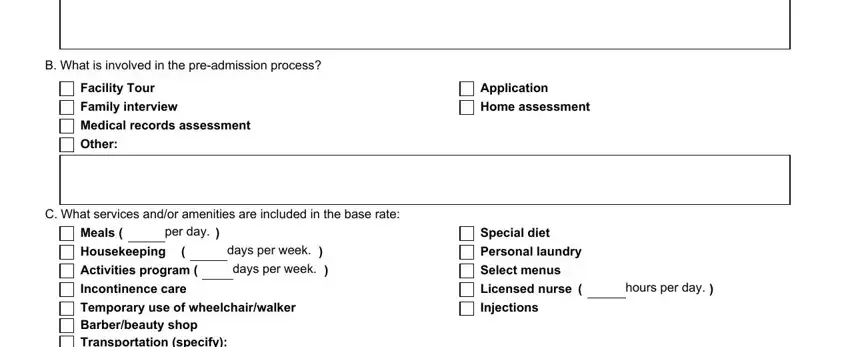
Fill out the B What is involved in the, Facility Tour, Family interview Medical records, Other, Application, Home assessment, C What services andor amenities, Meals, per day, Housekeeping Activities program, days per week days per week, Incontinence care Temporary use of, Special diet, Personal laundry Select menus, and Licensed nurse Injections space using the details required by the system.
In the Incontinence care Temporary use of part, describe the valuable details.

Inside the paragraph D What additional services can be, Beautybarber services, Incontinence care Incontinence, Injections, Other, Companion Transportation to doctor, Minor nursing services provided by, E Do you charge more for different, Yes, II Admission Process, A Does the facility have a written, B Is there a deposit in addition, If yes is it refundable, Yes, and Yes, identify the rights and responsibilities of the sides.
End by looking at the following sections and filling them in accordingly: Other, E Does the facility have, Staff who can sign for the deaf, Services for persons who are blind, Other, F Is there a trial period for new, Yes, If yes how long, III DischargeTransfer, A What could cause temporary, Medical condition requiring hour, Unacceptable physical or verbal, Drug stabilization, Other, and Resident requires services the.
Step 3: As you select the Done button, your finished document is simply transferable to any type of of your devices. Alternatively, you can easily send it using mail.
Step 4: Prepare duplicates of the file. This can protect you from potential misunderstandings. We do not check or distribute the information you have, so feel comfortable knowing it's going to be secure.
