Dap Note Sample PDF Details
The DAP Note Sample is a standardized form used by therapists, counselors, and mental health professionals. Each DAP note follows three sections: Data, Assessment, and Plan. Using a consistent dap note sample helps practitioners maintain accurate, organized clinical records across all client sessions.
What Each DAP Section Covers
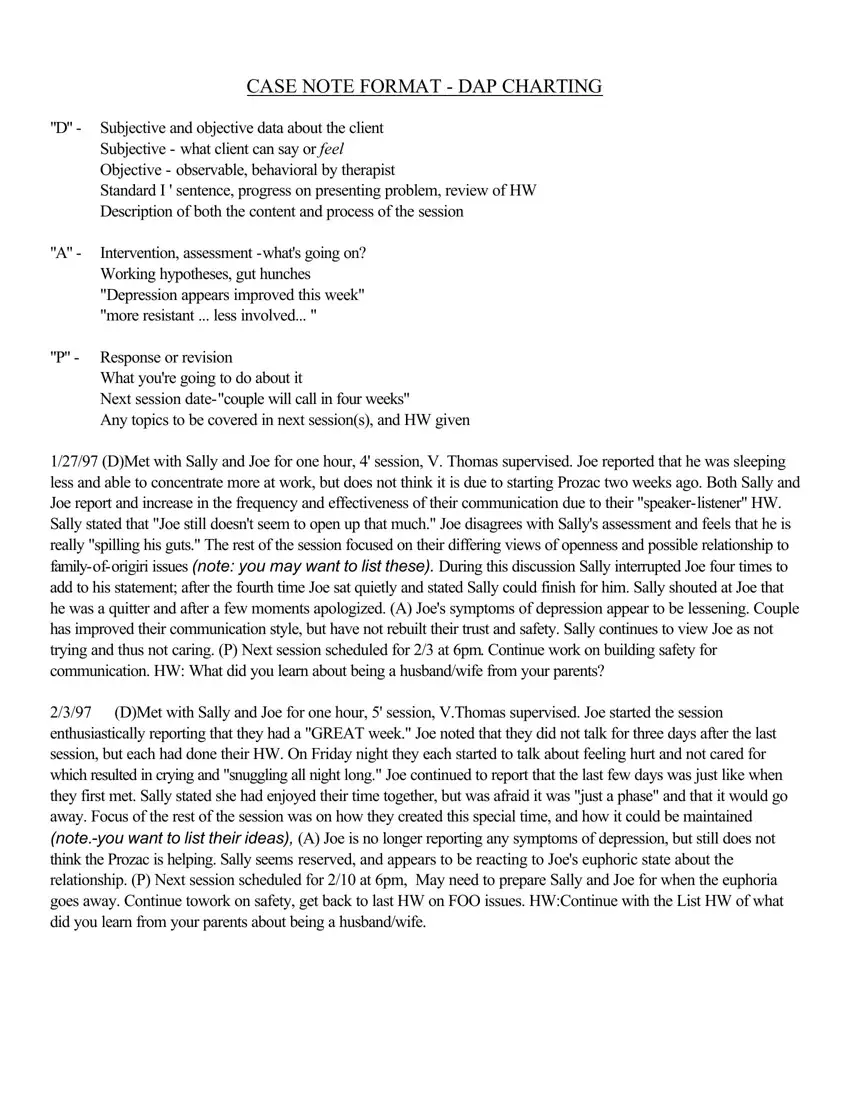
The Data (D) section records factual information about the session. It includes subjective data, meaning what the client reports about their mood or thoughts, and objective data, meaning behaviors the therapist directly observes. Only factual information belongs in this section. Do not add clinical interpretation to the Data section.
The Assessment (A) section captures the therapist's clinical conclusions. This includes progress observations, working diagnoses, and changes in the client's condition. For example, the therapist might note reduced anxiety, improved communication, or new coping strategies the client demonstrated during the session.
The Plan (P) section outlines what happens next in the treatment process. It includes the next session date, homework assigned to the client, referrals, and any changes to the treatment plan. Plan entries should be specific and measurable. Vague entries like "continue treatment" make it difficult to track progress over time.
Common Mistakes in DAP Note Documentation
Mixing the Data and Assessment sections is the most common documentation error. Therapists new to DAP format sometimes write their clinical interpretations inside the Data section. This reduces the clarity and objectivity of the note. Keep each section separate and focused on its defined purpose.
Leaving the Plan section incomplete is another frequent mistake. Every DAP note should include a concrete next step. Notes without a clear plan make handoff to other providers more difficult and disrupt continuity of care.
Writing overly long sentences in the Data section can make notes hard to read during future reviews. Use short, factual statements. Phrases like "client reported feeling overwhelmed at work" are cleaner than lengthy descriptions mixing multiple observations together.
Best Practices for DAP Note Completion
Complete each DAP note within 24 hours of the session. Prompt documentation keeps details accurate and reduces the risk of missing important clinical information.
Use short, precise sentences in each section. Write in the third person for consistency. Refer to the client's prior session notes to document progress or regression accurately over time.
A well-completed DAP note supports effective treatment planning, accurate insurance documentation, and coordination among care team members. Consistent use of a structured dap note sample improves documentation quality and protects both the therapist and client during any legal or insurance review.
| Question | Answer |
|---|
| Form Name | Dap Note Sample |
| Form Length | 5 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 15 sec |
| Other names | case note format sample, case note format, progress note generator, note format dap sample |