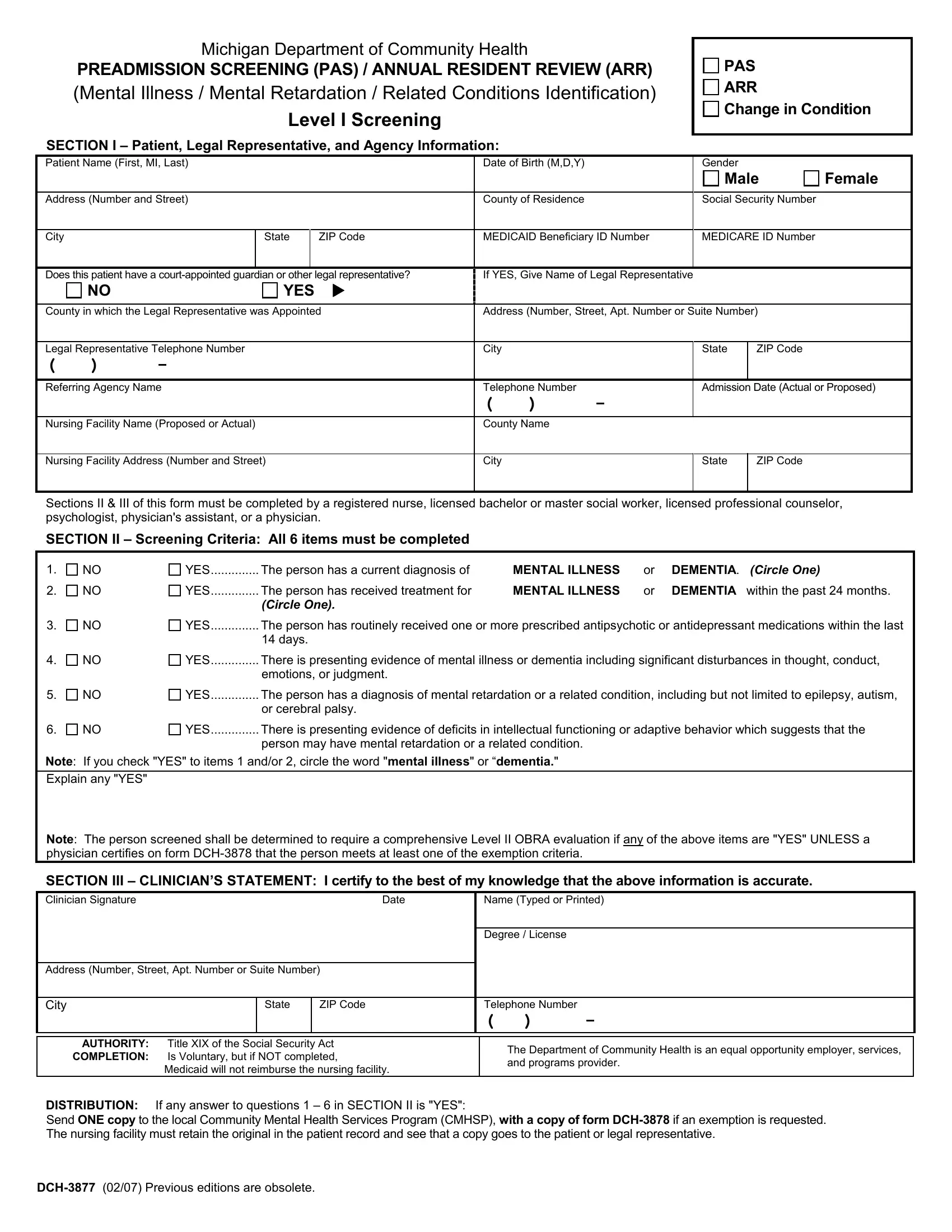
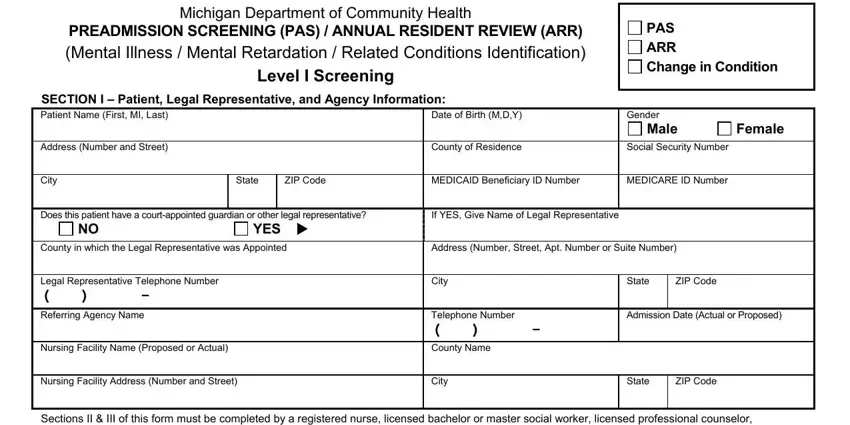
Michigan Department of Community Health
PREADMISSION SCREENING (PAS) / ANNUAL RESIDENT REVIEW (ARR)
(Mental Illness / Mental Retardation / Related Conditions Identification)
Level I Screening
SECTION I – Patient, Legal Representative, and Agency Information:
PAS
ARR
Change in Condition
Patient Name (First, MI, Last) |
|
Date of Birth (M,D,Y) |
|
Gender |
|
|
|
|
|
|
|
|
|
|
|
Male |
Female |
|
|
|
|
|
|
|
|
|
Address (Number and Street) |
|
County of Residence |
|
Social Security Number |
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
|
ZIP Code |
MEDICAID Beneficiary ID Number |
MEDICARE ID Number |
|
|
|
|
|
|
|
|
Does this patient have a court-appointed guardian or other legal representative? |
If YES, Give Name of Legal Representative |
|
|
|
|
NO |
|
YES |
|
|
|
|
|
|
|
|
|
|
|
County in which the Legal Representative was Appointed |
Address (Number, Street, Apt. Number or Suite Number) |
|
|
|
|
|
|
|
|
|
Legal Representative Telephone Number |
|
City |
|
|
State |
ZIP Code |
|
( |
) |
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Referring Agency Name |
|
Telephone Number |
|
Admission Date (Actual or Proposed) |
|
|
|
|
|
|
( |
) |
- |
|
|
|
|
|
|
|
|
|
|
Nursing Facility Name (Proposed or Actual) |
|
County Name |
|
|
|
|
|
|
|
|
|
|
|
|
Nursing Facility Address (Number and Street) |
|
City |
|
|
State |
ZIP Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
Sections II & III of this form must be completed by a registered nurse, licensed bachelor or master social worker, licensed professional counselor, psychologist, physician's assistant, or a physician.
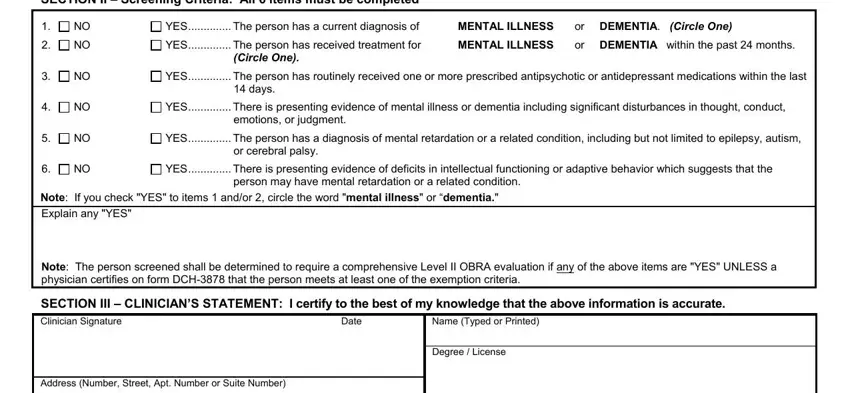
SECTION II – Screening Criteria: All 6 items must be completed
1. |
NO |
YES |
The person has a current diagnosis of |
MENTAL ILLNESS |
or |
DEMENTIA. (CIRCLE ONE) |
2. |
NO |
YES |
The person has received treatment for |
MENTAL ILLNESS |
or |
DEMENTIA within the past 24 months. |
|
|
|
(CIRCLE ONE). |
|
|
|
3. |
NO |
YES |
The person has routinely received one or more prescribed antipsychotic or antidepressant medications within the last |
|
|
|
14 days. |
|
|
|
4. |
NO |
YES |
There is presenting evidence of mental illness or dementia including significant disturbances in thought, conduct, |
|
|
|
emotions, or judgment. |
|
|
|
5. |
NO |
YES |
The person has a diagnosis of mental retardation or a related condition, including but not limited to epilepsy, autism, |
|
|
|
or cerebral palsy. |
|
|
|
6. |
NO |
YES |
There is presenting evidence of deficits in intellectual functioning or adaptive behavior which suggests that the |
|
|
|
person may have mental retardation or a related condition. |
|
|
Note: If you check "YES" to items 1 and/or 2, circle the word "mental illness" or “dementia."
Explain any "YES"
Note: The person screened shall be determined to require a comprehensive Level II OBRA evaluation if any of the above items are "YES" UNLESS a physician certifies on form DCH-3878 that the person meets at least one of the exemption criteria.
SECTION III – CLINICIAN’S STATEMENT: I certify to the best of my knowledge that the above information is accurate.
Clinician Signature |
|
|
Date |
|
Name (Typed or Printed) |
|
|
|
|
|
|
|
|
|
|
|
|
Degree / License |
|
|
|
|
|
|
|
|
Address (Number, Street, Apt. Number or Suite Number) |
|
|
|
|
|
|
|
|
|
|
|
City |
|
State |
ZIP Code |
|
Telephone Number |
|
|
|
|
|
( |
) |
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AUTHORITY: |
Title XIX of the Social Security Act |
|
|
The Department of Community Health is an equal opportunity employer, services, |
COMPLETION: |
Is Voluntary, but if NOT completed, |
|
|
|
|
and programs provider. |
|
Medicaid will not reimburse the nursing facility. |
|
|
|
|
|
|
|
DISTRIBUTION: If any answer to questions 1 – 6 in SECTION II is "YES":
Send ONE copy to the local Community Mental Health Services Program (CMHSP), with a copy of form DCH-3878 if an exemption is requested. The nursing facility must retain the original in the patient record and see that a copy goes to the patient or legal representative.
DCH-3877 (02/07) Previous editions are obsolete.
Mental Illness / Mental Retardation / Related Condition Identification Criteria
Instructions for DCH-3877
The DCH-3877 is used to identify prospective and current nursing facility residents who meet the criteria for possible mental illness or mental retardation, or a related condition and who may be in need of mental health services.
Sections II and III must be completed by a registered nurse, licensed bachelor or master social worker, licensed professional counselor, psychologist, physician’s assistant, or physician.
Preadmission Screening: The DCH-3877 must be completed by hospitals as part of the discharge planning process or by physicians seeking to admit an individual to a nursing facility from other than an acute care setting. Check the PAS box.
Annual resident review: The DCH-3877 must be completed by the nursing facility. Check the ARR box.
Section II – Screening Criteria – All 6 items on the form must be completed. The following provides additional explanation of the items.
1.Mental Illness: A current primary diagnosis of a mental disorder as defined in the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revised (DSM-IV-TR™).
Current Diagnosis means that a physician has established a diagnosis of a mental disorder within the past twenty-four
(24)months. Do NOT mark “YES” for an individual cited as having a diagnosis "by history" only.
2.Receipt of treatment for mental illness or dementia within the past 24 months means any of the following: inpatient psychiatric hospitalization; outpatient services such as psychotherapy, day program, or mental health case management; or referral for psychiatric consultation, evaluation, or prescription of psychopharmacological medications.
3.Antidepressant and antipsychotic medications mean any currently prescribed medication classified as an antidepressant or antipsychotic, plus Lithium Carbonate and Lithium Citrate.
4.Presenting evidence means the individual currently manifests symptoms of mental illness or dementia, which suggest the need for further evaluation to establish causal factors, diagnosis and treatment recommendations.
5.Mental Retardation / Related Condition: An individual is considered to have a severe, chronic disability that meets ALL four (4) of the following conditions:
a) It is manifested before the person reaches age 22. b) It is likely to continue indefinitely.
c) It results in substantial functional limitations in 3 or more of the following areas of major life activity: self-care, understanding and use of language, learning, mobility, self-direction, and capacity for independent living.
d) It is attributable to:
•mental retardation such that the person has significant subaverage general intellectual functioning existing concurrently with deficits in adaptive behavior and manifested during the developmental period;
•cerebral palsy, epilepsy, autism; or
•any condition other than mental illness found to be closely related to mental retardation because this condition results in impairment in general intellectual functioning OR adaptive behavior similar to that of persons with mental retardation, and requires treatment or services similar to those required for these persons.
6.Presenting evidence means the individual manifests deficits in intellectual functioning or adaptive behavior, which suggests the need for further evaluation to determine presence of a developmental disability, causal factors, and treatment recommendations.
NOTE: When there is one or more "YES" answers to questions 1 – 6 under SECTION II, a Mental Illness / Mental Retardation / Related Condition Exemption Criteria Certification, DCH-3878 must be completed only if the referring agency is seeking to establish exemption criteria for a dementia, state of coma, or hospital exempted discharge.
DCH-3877 (02/07) Previous editions are obsolete.