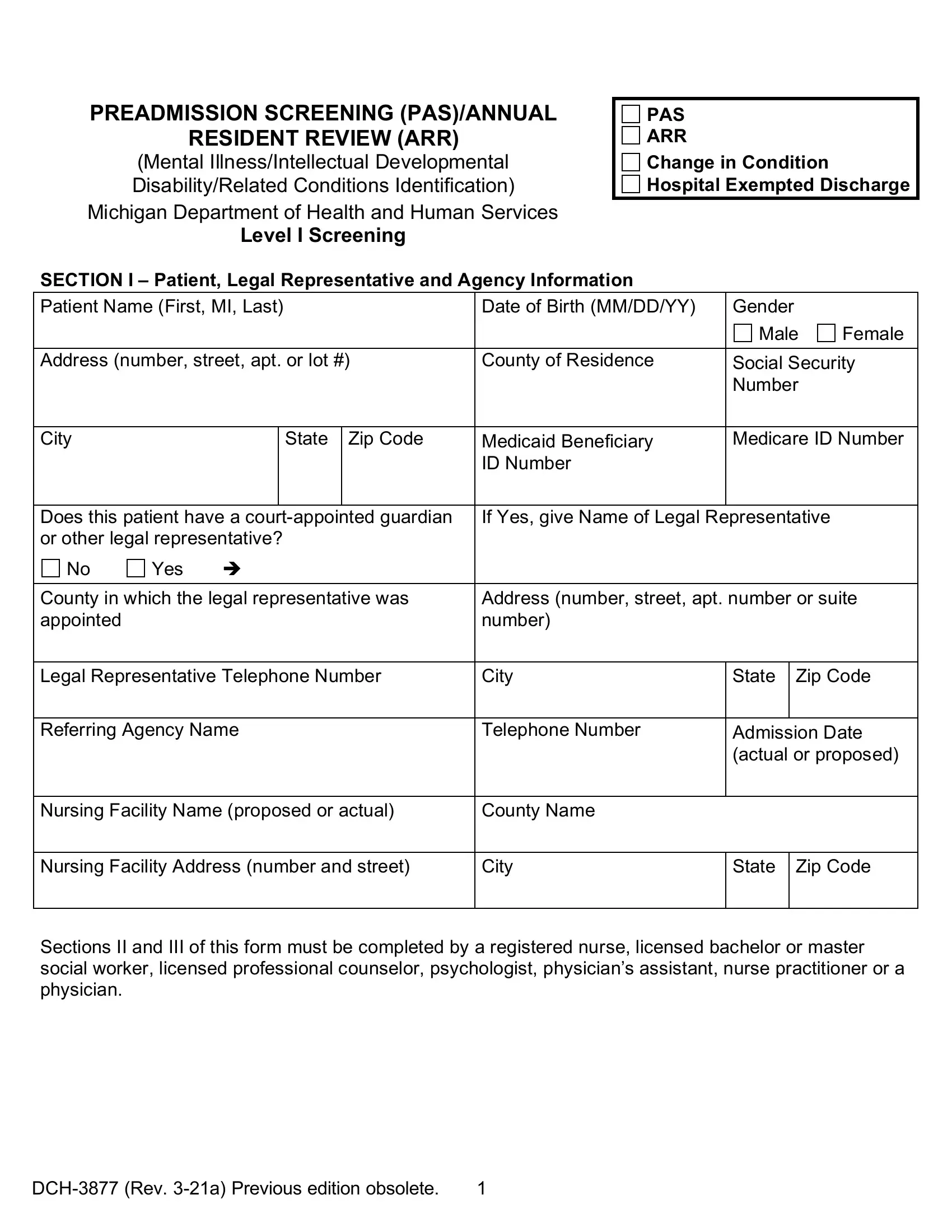
In navigating the complexities of healthcare and mental health services within Michigan, the Michigan Department of Community Health has introduced specific forms, namely the DCH-3877 and DCH-3878, to streamline processes for Medicaid beneficiaries. These forms play a critical role in the preadmission screening (PAS) and annual resident review (ARR) for individuals exhibiting signs of mental illness or developmental disability, ensuring they receive the appropriate level of care. The DCH-3877 form is utilized to identify those prospective and current nursing facility residents who may require mental health services, requiring completion by qualified health professionals. This meticulous process demands accurate diagnosis and detailed patient history to ensure the provision of essential services and support. Similarly, the DCH-3878 form seeks to certify criteria for exemptions, further emphasizing the state's commitment to tailored healthcare provisions. The revision of these forms, effective July 1, 2003, signifies an ongoing effort to better address the needs of the community, updating criteria and terminologies to align with contemporary standards. This commitment is further demonstrated through the structured distribution and easy accessibility of these forms, aiming to facilitate a seamless interface between healthcare providers, patients, and the Medicaid system. Understanding the function and requirements of these forms is crucial for healthcare providers, patients, and their families to navigate the Medicaid system effectively, ensure compliance, and secure the necessary care and support for those with mental illnesses or developmental disabilities.
| Question | Answer |
|---|---|
| Form Name | Michigan Dch 3877 Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | form 3877 mi mental illness, dch 3878 form, dch3877, dch 3877 printable |