
You are able to fill out dd form 1172 id card easily in our PDFinity® online tool. To make our tool better and more convenient to utilize, we consistently develop new features, with our users' feedback in mind. If you are seeking to get going, here's what you will need to do:
Step 1: Hit the "Get Form" button at the top of this webpage to get into our tool.
Step 2: As soon as you launch the online editor, you'll notice the form prepared to be filled in. Aside from filling in various fields, you could also do many other actions with the Document, including putting on your own words, changing the initial textual content, inserting graphics, placing your signature to the PDF, and a lot more.
This PDF form will involve some specific details; to ensure accuracy and reliability, you need to heed the guidelines below:
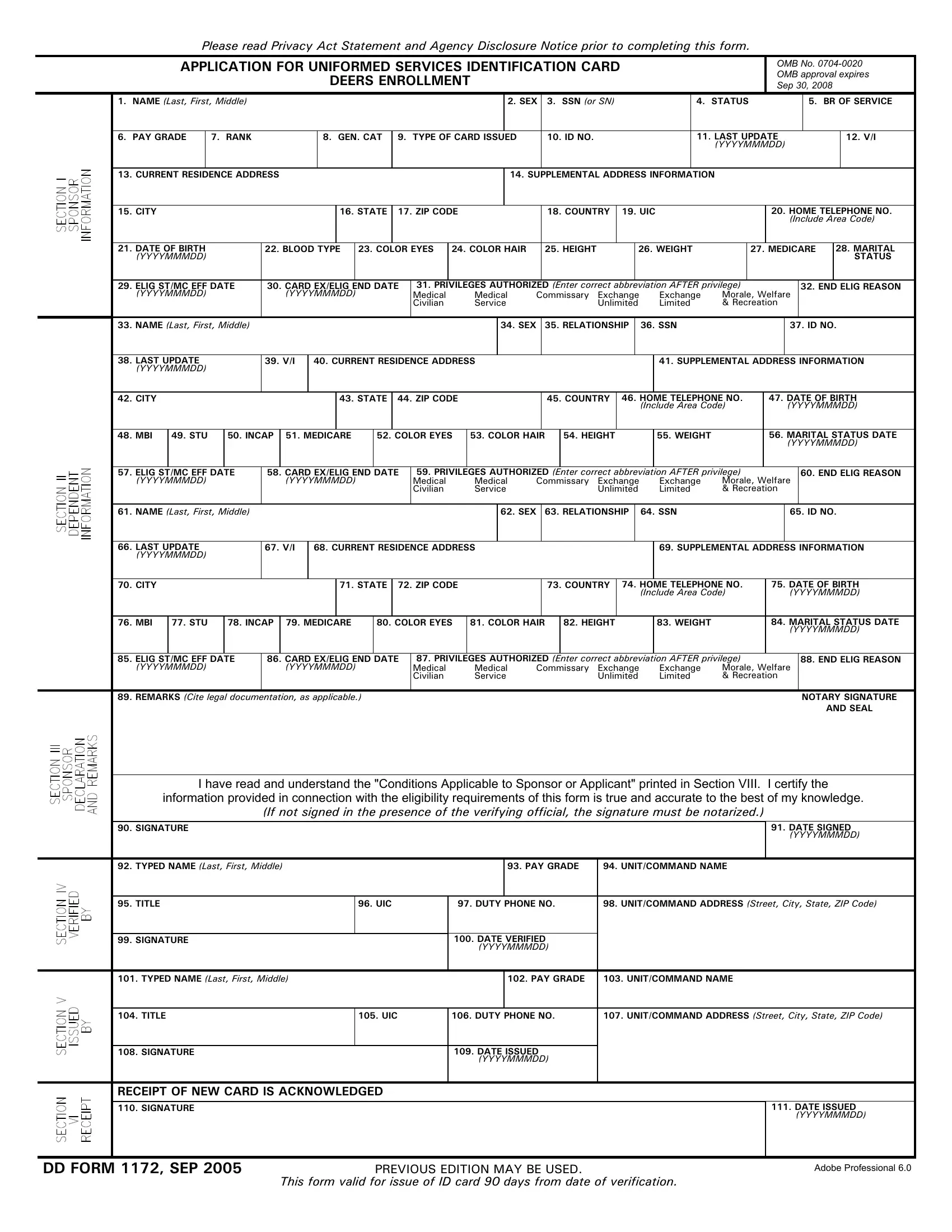
1. You should complete the dd form 1172 id card accurately, therefore be mindful when working with the areas that contain all of these blank fields:
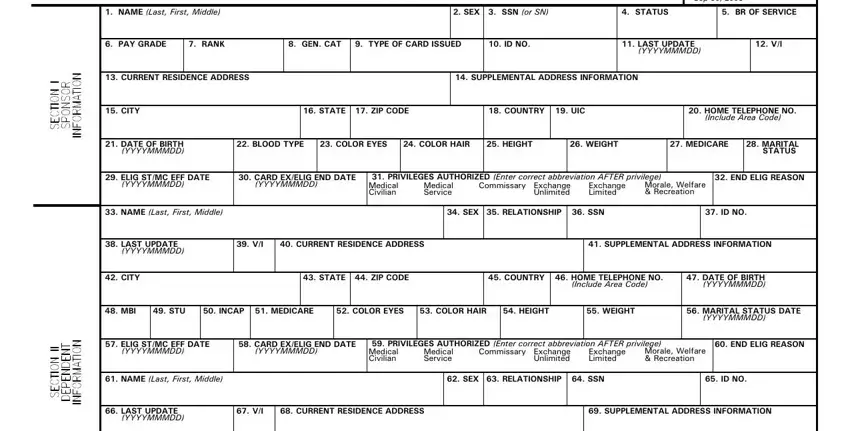
2. Right after filling out the previous section, head on to the subsequent step and complete the essential particulars in all these blanks - CITY, STATE ZIP CODE, COUNTRY HOME TELEPHONE NO, Include Area Code, DATE OF BIRTH YYYYMMMDD, MBI, STU, INCAP MEDICARE, COLOR EYES, COLOR HAIR, HEIGHT, WEIGHT, MARITAL STATUS DATE, YYYYMMMDD, and ELIG STMC EFF DATE.
3. This next stage is simple - fill out all the blanks in UNITCOMMAND ADDRESS Street City, SIGNATURE, DATE ISSUED, YYYYMMMDD, RECEIPT OF NEW CARD IS, DATE ISSUED, YYYYMMMDD, DD FORM SEP, This form valid for issue of ID, PREVIOUS EDITION MAY BE USED, and Adobe Professional to conclude this part.
Concerning DATE ISSUED and SIGNATURE, ensure that you don't make any mistakes in this current part. Both these could be the most important ones in the document.
Step 3: Right after looking through the form fields you have filled in, hit "Done" and you're done and dusted! After registering afree trial account here, you will be able to download dd form 1172 id card or email it immediately. The PDF will also be easily accessible in your personal account page with all your changes. FormsPal offers secure document tools with no personal data recording or sharing. Feel safe knowing that your details are in good hands with us!