The process of completing the dd form 2492 is actually straightforward. We ensured our software is not hard to understand and can help fill in any kind of PDF within minutes. Have a look at several steps you will have to take:
Step 1: Look for the button "Get Form Here" on this site and next, click it.
Step 2: Now, you can start editing the dd form 2492. The multifunctional toolbar is at your disposal - insert, remove, change, highlight, and undertake other commands with the content material in the document.
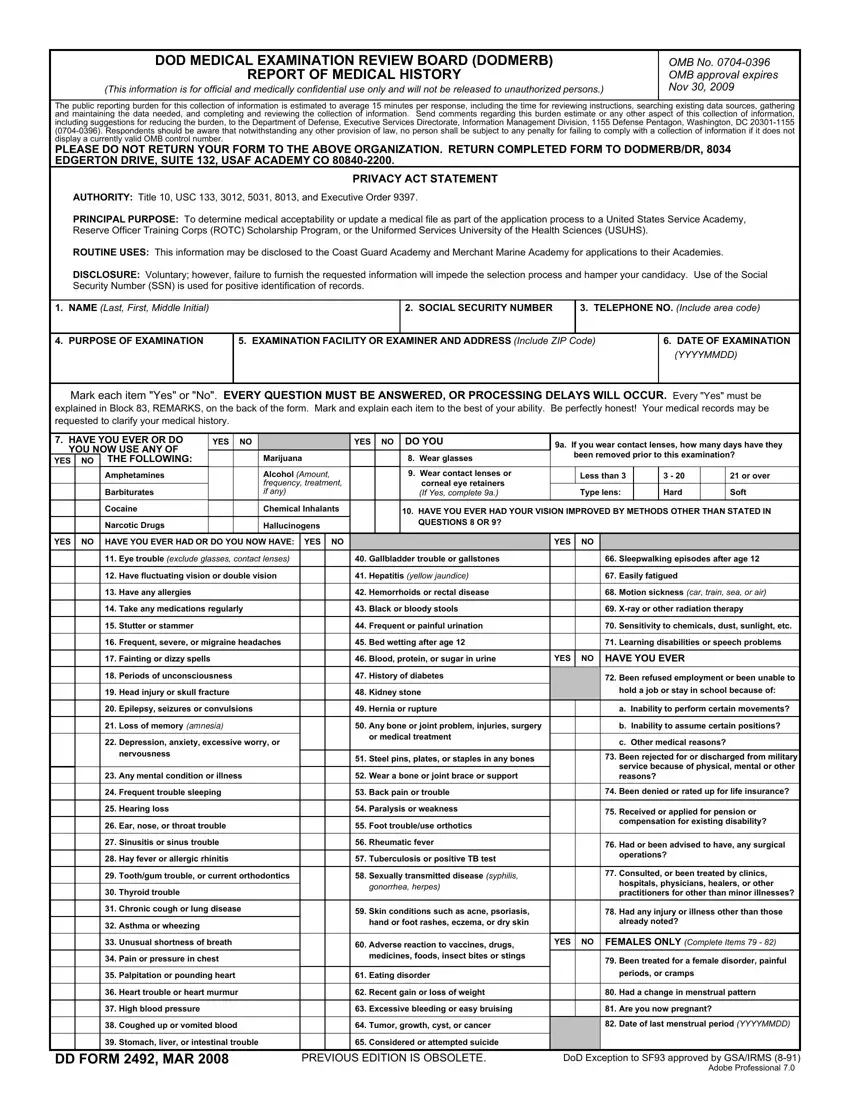
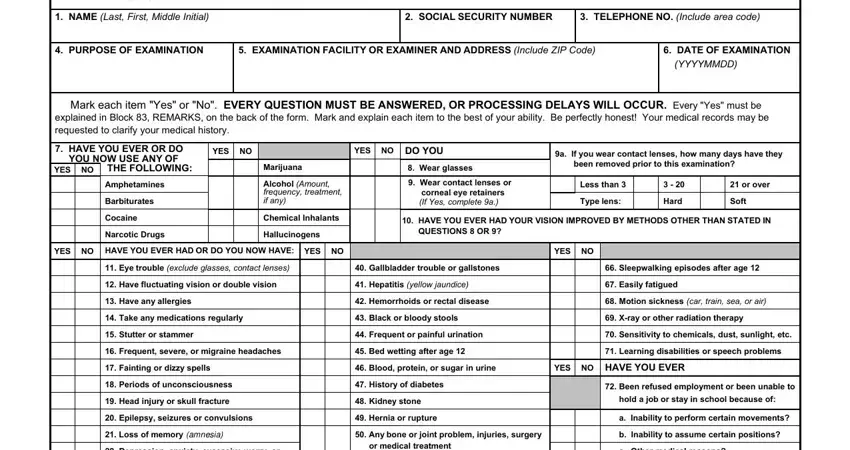
Enter the information required by the program to get the form.
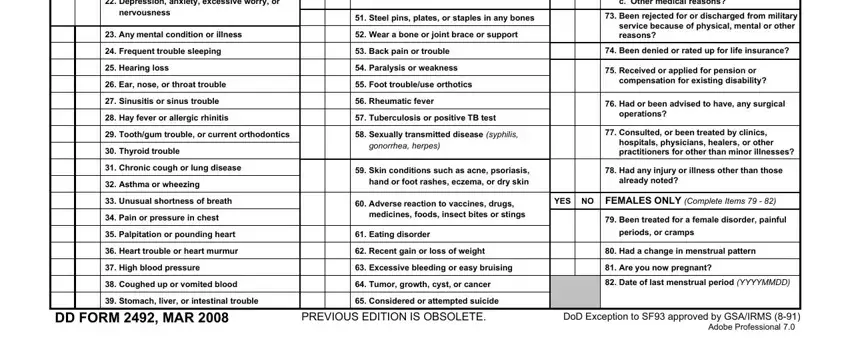
Write the necessary information in the Depression anxiety excessive, Any bone or joint problem, Steel pins plates or staples in, Any mental condition or illness, Wear a bone or joint brace or, Frequent trouble sleeping, Hearing loss, Ear nose or throat trouble, Sinusitis or sinus trouble, Back pain or trouble, Paralysis or weakness, Foot troubleuse orthotics, Rheumatic fever, Hay fever or allergic rhinitis, and Tuberculosis or positive TB test area.
The software will require you to present particular important data to effortlessly fill out the section REMARKS Applicant use only Every.
The TYPED OR PRINTED NAME OF, SIGNATURE OF EXAMINEEAPPLICANT, DATE SIGNED YYYYMMDD, EXAMINERS SUMMARY AND ELABORATION, EXAMINER TYPED OR PRINTED NAME OF, SIGNATURE OF EXAMINER, DATE SIGNED YYYYMMDD, and NUMBER OF ATTACHED SHEETS field will be your place to insert the rights and obligations of either side.
Step 3: Choose the Done button to save the file. So now it is ready for export to your gadget.
Step 4: To stay away from probable forthcoming concerns, be sure to possess as much as several copies of any document.
