
If you would like to fill out 2000, you don't need to download any kind of programs - just make use of our online PDF editor. We at FormsPal are focused on making sure you have the ideal experience with our tool by continuously releasing new capabilities and upgrades. Our editor has become much more useful as the result of the most recent updates! So now, editing PDF documents is simpler and faster than before. Here's what you'd need to do to get started:
Step 1: Access the PDF inside our editor by clicking on the "Get Form Button" at the top of this webpage.
Step 2: The editor offers the ability to modify almost all PDF documents in various ways. Improve it by including personalized text, adjust what's originally in the PDF, and include a signature - all within the reach of a couple of clicks!
When it comes to blank fields of this specific PDF, here's what you need to do:
1. Fill out your 2000 with a selection of essential blanks. Consider all of the necessary information and make certain there is nothing forgotten!
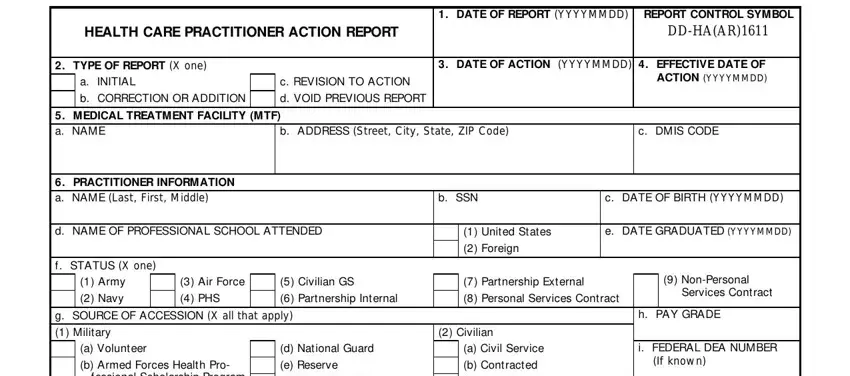
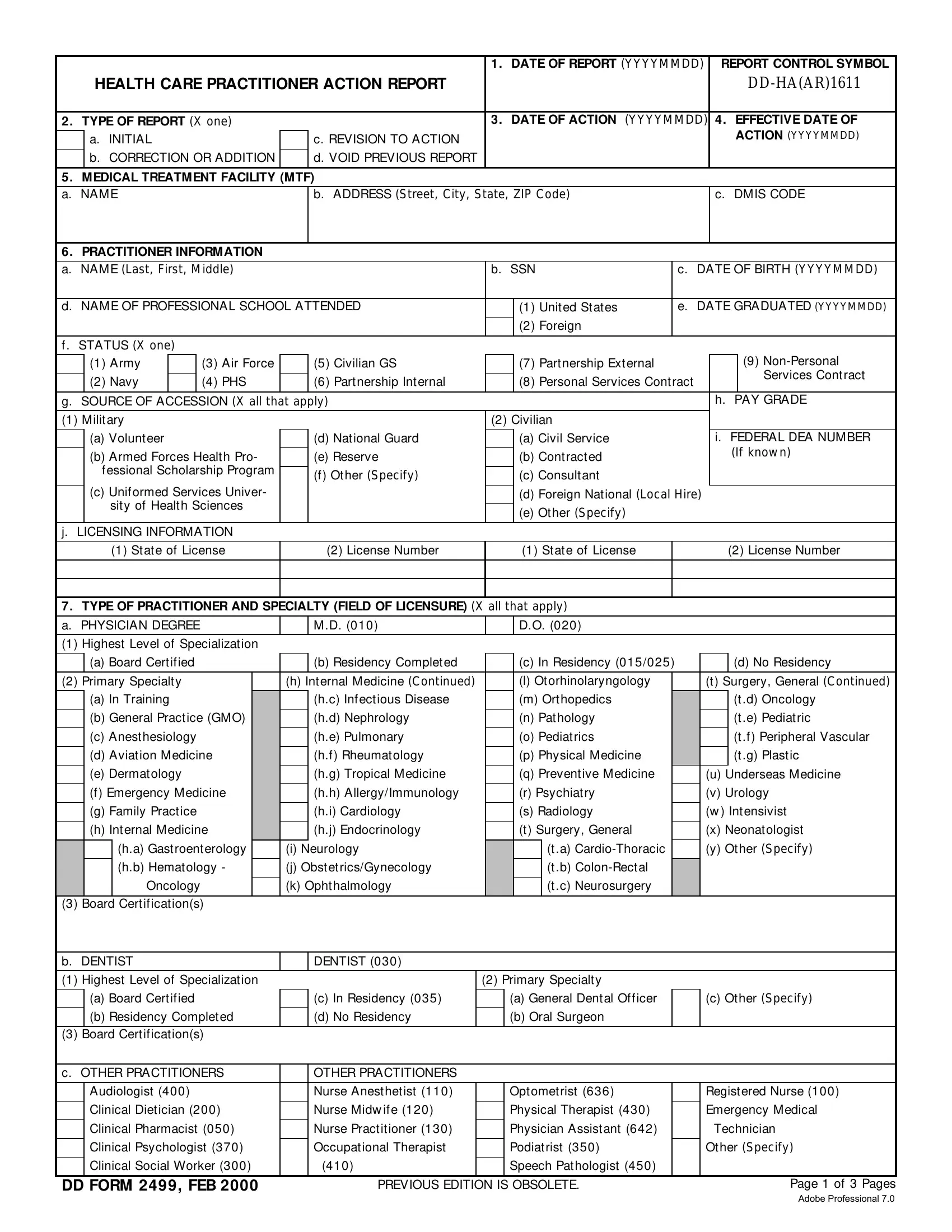
2. The next part would be to submit these blanks: b Armed Forces Health Pro, c Uniformed Services Univer sity, j LICENSING INFORMATION, e Reserve f Other Specify, c Consultant d Foreign National, State of License, License Number, State of License, License Number, TYPE OF PRACTITIONER AND, Highest Level of Specialization, a Board Certified, b Residency Completed, c In Residency, and d No Residency.
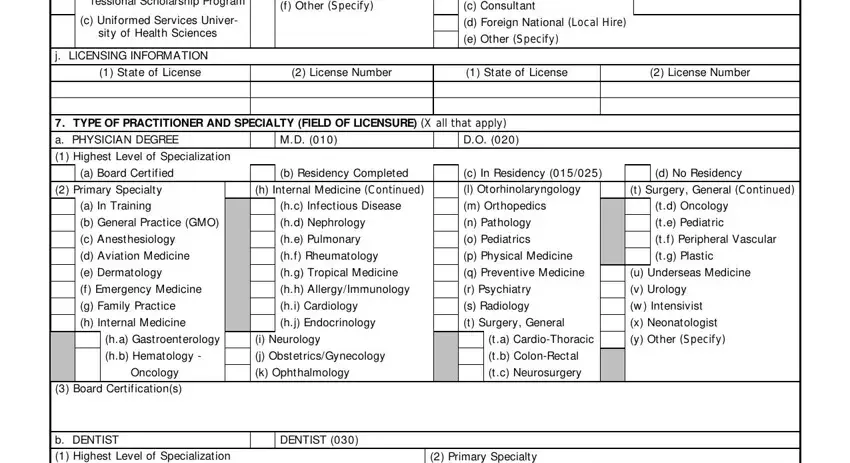
3. Completing Highest Level of Specialization, Primary Specialty, a Board Certified, c In Residency, a General Dental Officer, c Other Specify, b Residency Completed, d No Residency, b Oral Surgeon, Board Certifications, c OTHER PRACTITIONERS, OTHER PRACTITIONERS, Audiologist, Nurse Anesthetist, and Optometrist is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. You're ready to start working on this next part! Here you have all of these a PRIVILEGING ACTIONS TAKENREASON, b ACTIONS OTHER THAN PRIVILEGING, c LENGTH OF ACTION In months, NONE, NONE, d LIST HOW AND WHY WHAT PRIVILEGES, e OTHER ACTIONS TAKEN X all that, Review, Separated for Cause, Separated, Rehabilitation, OntheJob Training, FiredTerminated, Resigned, and CIVILIAN CONTRACTOR NAME blank fields to complete.
People frequently make mistakes when completing c LENGTH OF ACTION In months in this part. Ensure you double-check whatever you type in right here.
5. This last notch to finalize this PDF form is critical. Make certain you fill in the necessary form fields, like REMARKS, OFFICE OF THE SURGEON GENERAL, b TITLE, d ADDRESS Office of the, Surgeon General, e SIGNATURE, c TELEPHONE NUMBER, f DATE SIGNED YYYYMMDD, INSTRUCTIONS, All other items are selfexplanatory, and b Correction or Addition An, before submitting. Failing to do this can result in an unfinished and possibly nonvalid form!
Step 3: Ensure that the information is correct and then click "Done" to continue further. Create a 7-day free trial option with us and acquire instant access to 2000 - download or modify from your FormsPal account page. Whenever you work with FormsPal, you can fill out forms without having to be concerned about personal data leaks or entries getting distributed. Our protected platform helps to ensure that your personal data is kept safely.