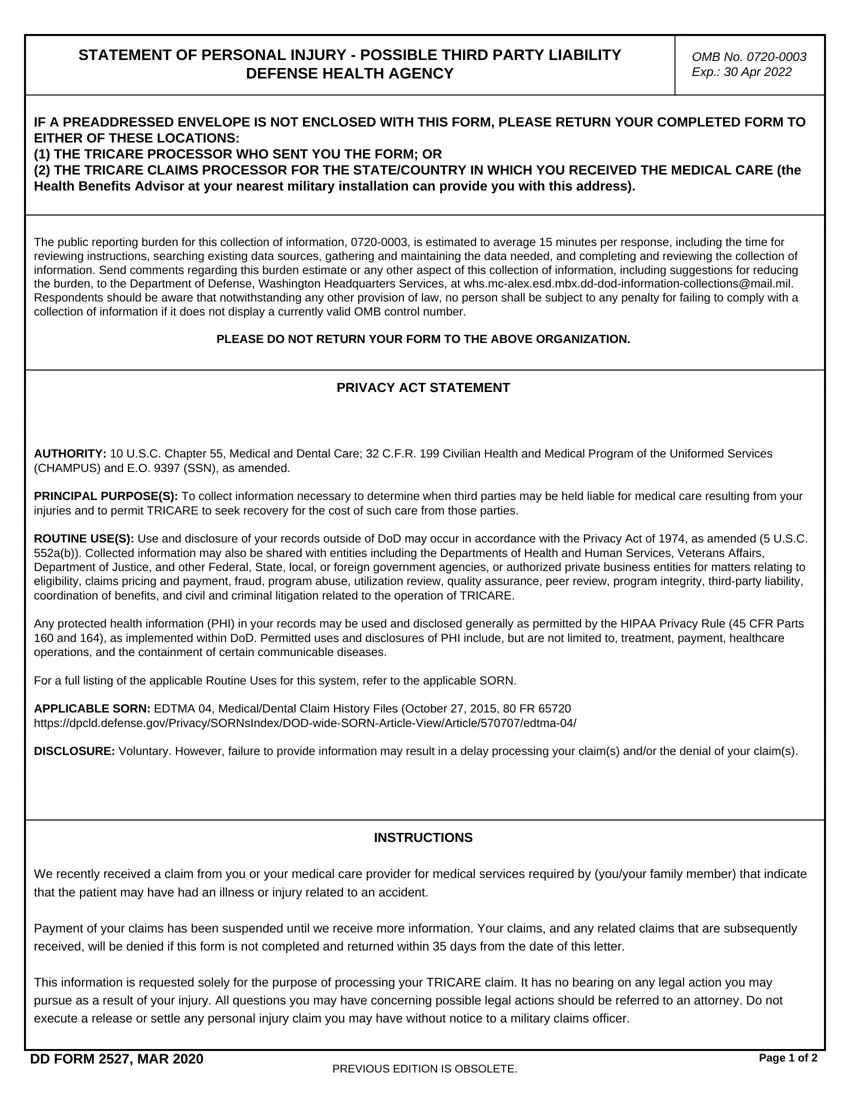
IF A PREADDRESSED ENVELOPE IS NOT ENCLOSED WITH THIS FORM, PLEASE RETURN YOUR COMPLETED FORM TO EITHER OF THESE LOCATIONS:
(1)THE TRICARE PROCESSOR WHO SENT YOU THE FORM; OR
(2)THE TRICARE CLAIMS PROCESSOR FOR THE STATE/COUNTRY IN WHICH YOU RECEIVED THE MEDICAL CARE (the Health Benefits Advisor at your nearest military installation can provide you with this address).
The public reporting burden for this collection of information, 0720-0003, is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing the burden, to the Department of Defense, Washington Headquarters Services, at whs.mc-alex.esd.mbx.dd-dod-information-collections@mail.mil. Respondents should be aware that notwithstanding any other provision of law, no person shall be subject to any penalty for failing to comply with a collection of information if it does not display a currently valid OMB control number.
PLEASE DO NOT RETURN YOUR FORM TO THE ABOVE ORGANIZATION.
PRIVACY ACT STATEMENT
AUTHORITY: 10 U.S.C. Chapter 55, Medical and Dental Care; 32 C.F.R. 199 Civilian Health and Medical Program of the Uniformed Services (CHAMPUS) and E.O. 9397 (SSN), as amended.
PRINCIPAL PURPOSE(S): To collect information necessary to determine when third parties may be held liable for medical care resulting from your injuries and to permit TRICARE to seek recovery for the cost of such care from those parties.
ROUTINE USE(S): Use and disclosure of your records outside of DoD may occur in accordance with the Privacy Act of 1974, as amended (5 U.S.C. 552a(b)). Collected information may also be shared with entities including the Departments of Health and Human Services, Veterans Affairs, Department of Justice, and other Federal, State, local, or foreign government agencies, or authorized private business entities for matters relating to eligibility, claims pricing and payment, fraud, program abuse, utilization review, quality assurance, peer review, program integrity, third-party liability, coordination of benefits, and civil and criminal litigation related to the operation of TRICARE.
Any protected health information (PHI) in your records may be used and disclosed generally as permitted by the HIPAA Privacy Rule (45 CFR Parts 160 and 164), as implemented within DoD. Permitted uses and disclosures of PHI include, but are not limited to, treatment, payment, healthcare operations, and the containment of certain communicable diseases.
For a full listing of the applicable Routine Uses for this system, refer to the applicable SORN.
APPLICABLE SORN: EDTMA 04, Medical/Dental Claim History Files (October 27, 2015, 80 FR 65720 https://dpcld.defense.gov/Privacy/SORNsIndex/DOD-wide-SORN-Article-View/Article/570707/edtma-04/
DISCLOSURE: Voluntary. However, failure to provide information may result in a delay processing your claim(s) and/or the denial of your claim(s).
INSTRUCTIONS
We recently received a claim from you or your medical care provider for medical services required by (you/your family member) that indicate that the patient may have had an illness or injury related to an accident.
Payment of your claims has been suspended until we receive more information. Your claims, and any related claims that are subsequently received, will be denied if this form is not completed and returned within 35 days from the date of this letter.
This information is requested solely for the purpose of processing your TRICARE claim. It has no bearing on any legal action you may pursue as a result of your injury. All questions you may have concerning possible legal actions should be referred to an attorney. Do not execute a release or settle any personal injury claim you may have without notice to a military claims officer.