
dd form 2656 5 aug 2011 can be completed online easily. Simply make use of FormsPal PDF editor to get it done without delay. To keep our editor on the forefront of practicality, we work to put into practice user-driven capabilities and enhancements regularly. We are routinely grateful for any suggestions - join us in revampimg PDF editing. Here's what you'd need to do to start:
Step 1: Just click the "Get Form Button" at the top of this site to open our pdf editor. Here you will find everything that is needed to work with your document.
Step 2: As soon as you open the tool, you will see the form made ready to be filled out. Other than filling in various fields, you can also do other sorts of things with the Document, that is putting on your own textual content, modifying the initial textual content, inserting images, placing your signature to the form, and more.
It is actually easy to fill out the document with our helpful tutorial! This is what you have to do:
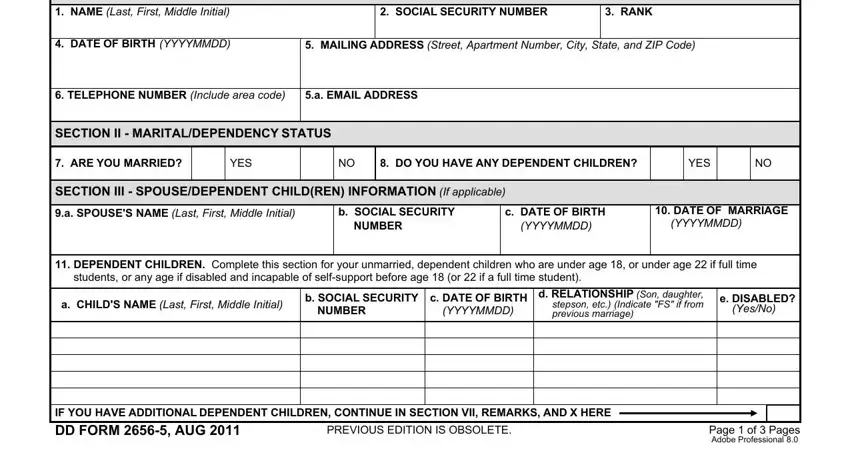
1. The dd form 2656 5 aug 2011 needs specific details to be entered. Ensure that the subsequent blank fields are filled out:
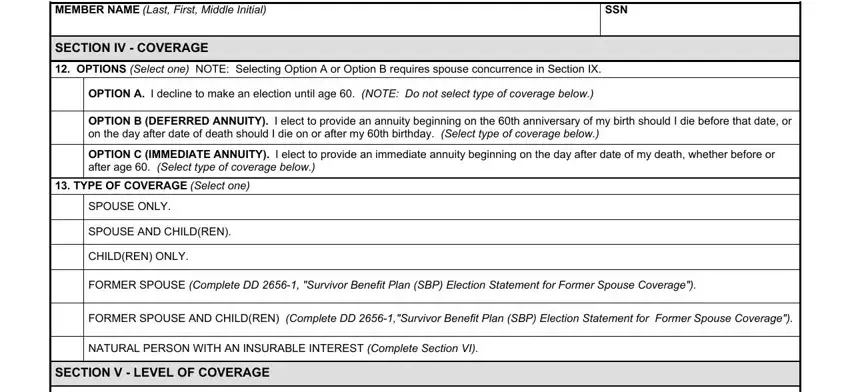
2. After performing this section, go on to the subsequent stage and fill out the necessary details in these blanks - MEMBER NAME Last First Middle, SSN, SECTION IV COVERAGE, OPTIONS Select one NOTE Selecting, OPTION A I decline to make an, OPTION B DEFERRED ANNUITY I elect, OPTION C IMMEDIATE ANNUITY I elect, TYPE OF COVERAGE Select one, SPOUSE ONLY, SPOUSE AND CHILDREN, CHILDREN ONLY, FORMER SPOUSE Complete DD, FORMER SPOUSE AND CHILDREN, NATURAL PERSON WITH AN INSURABLE, and SECTION V LEVEL OF COVERAGE.
3. In this step, look at Select the monthly amount of, FULL RETIRED PAY, REDUCED AMOUNT OF RETIRED PAY, NOTE Spouse concurrence required, SECTION VI INSURABLE INTEREST, INSURABLE INTEREST BENEFICIARY a, b SOCIAL SECURITY NUMBER, c DATE OF BIRTH YYYYMMDD, d MAILING ADDRESS Street Apartment, e RELATIONSHIP TO MEMBER, SECTION VII REMARKS, and USE THIS SECTION TO CONTINUE AN. All of these should be filled in with highest precision.
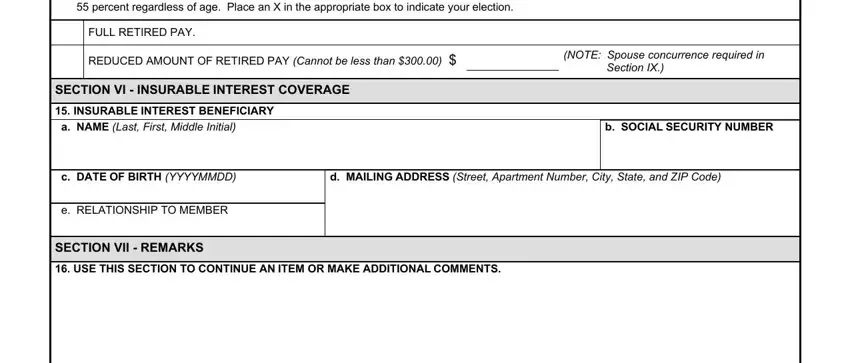
Regarding SECTION VI INSURABLE INTEREST and Select the monthly amount of, ensure you take a second look here. Both of these are the most important fields in the PDF.
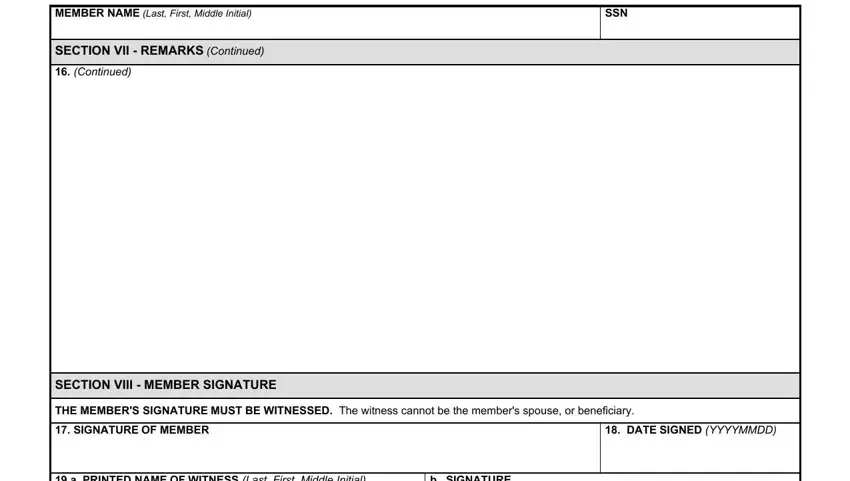
4. It's time to fill in this next segment! Here you will have all of these MEMBER NAME Last First Middle, SSN, SECTION VII REMARKS Continued, Continued, SECTION VIII MEMBER SIGNATURE, THE MEMBERS SIGNATURE MUST BE, SIGNATURE OF MEMBER, DATE SIGNED YYYYMMDD, a PRINTED NAME OF WITNESS Last, and b SIGNATURE form blanks to fill in.
5. The last point to finish this form is crucial. Make sure to fill in the necessary form fields, including a PRINTED NAME OF WITNESS Last, b SIGNATURE, c MAILING ADDRESS OF WITNESS, d DATE SIGNED YYYYMMDD, SECTION IX SPOUSE CONCURRENCE, Spousal consent and signature are, SPOUSE I hereby consent in my, a SIGNATURE, b DATE SIGNED YYYYMMDD, NOTARY WITNESS, On this, day of, and before me the undersigned notary, before finalizing. If you don't, it could contribute to a flawed and probably invalid document!
Step 3: Always make sure that the information is accurate and then just click "Done" to finish the project. Find the dd form 2656 5 aug 2011 the instant you subscribe to a free trial. Immediately gain access to the pdf document from your personal account, with any modifications and adjustments being all kept! FormsPal is dedicated to the privacy of our users; we always make sure that all information used in our editor is protected.