
You can prepare INCAPACITATION without difficulty with the help of our PDFinity® PDF editor. Our tool is consistently evolving to provide the best user experience possible, and that is due to our commitment to continuous development and listening closely to user opinions. Should you be looking to start, this is what it takes:
Step 1: Just press the "Get Form Button" above on this site to open our pdf form editing tool. There you will find all that is needed to work with your document.
Step 2: With our advanced PDF tool, it's possible to do more than just complete blanks. Edit away and make your forms look faultless with customized textual content put in, or modify the original input to perfection - all comes along with an ability to incorporate just about any photos and sign the PDF off.
When it comes to blank fields of this particular form, this is what you need to know:
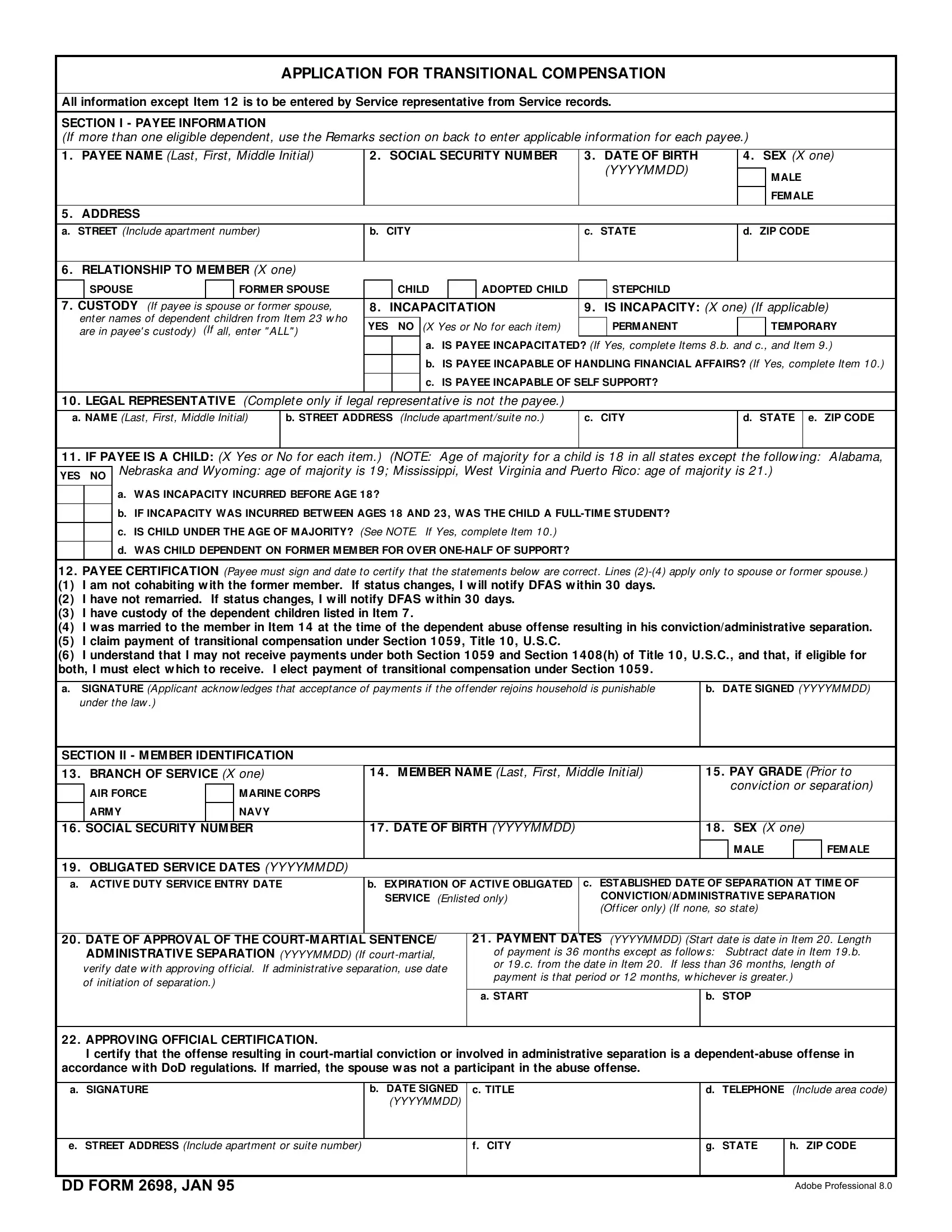
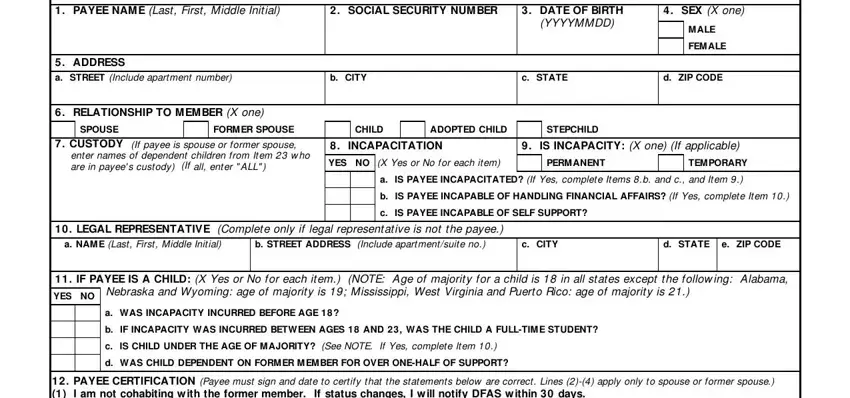
1. Complete your INCAPACITATION with a number of essential blank fields. Note all of the necessary information and make certain nothing is neglected!
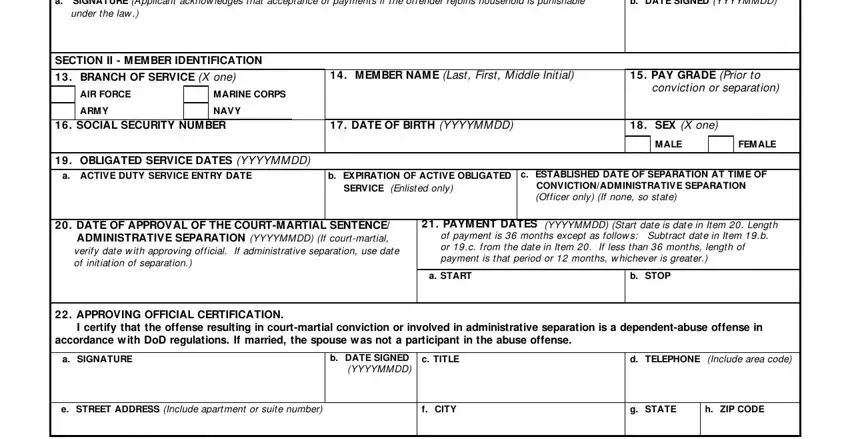
2. Once the previous segment is completed, you have to include the needed details in SIGNATURE under the law, Applicant acknow ledges that, b DATE SIGNED YYYYMMDD, SECTION II M EM BER IDENTIFICATION, BRANCH OF, SERVICE X one, AIR FORCE, ARM Y, M ARINE CORPS, NAVY, M EM BER NAM E, Last First Middle Initial, PAY GRADE Prior to, conviction or separation, and SOCIAL SECURITY NUM BER allowing you to proceed to the 3rd part.
3. Within this stage, have a look at NAM E Last First Middle Initial, SOCIAL SECURITY NUM BER, DATE OF BIRTH YYYYMMDD, and SECTION III REMARKS Use this area. Each one of these must be completed with highest accuracy.
People often make errors while filling out SOCIAL SECURITY NUM BER in this section. Don't forget to reread what you enter right here.
4. Now fill out this fourth portion! In this case you will have all these SECTION IV APPROPRIATION DATA, FUND CITE APPROVING OFFICIAL, a SIGNATURE, b DATE SIGNED YYYYMMDD, c TITLE, d TELEPHONE Include area code, e STREET ADDRESS Include apartment, f CITY, g STATE, h ZIP CODE, and DD FORM BACK JAN blank fields to fill in.
Step 3: Prior to moving on, double-check that form fields are filled in properly. As soon as you’re satisfied with it, click “Done." After registering a7-day free trial account at FormsPal, you will be able to download INCAPACITATION or send it via email directly. The PDF will also be easily accessible via your personal account menu with all of your changes. FormsPal guarantees your information privacy via a secure system that never records or shares any sort of private information typed in. Feel safe knowing your documents are kept protected each time you work with our editor!