
Any time you need to fill out DD Form 2813 fillable, you don't have to download and install any sort of applications - just give a try to our online tool. To make our editor better and easier to work with, we continuously work on new features, with our users' suggestions in mind. Here is what you would want to do to begin:
Step 1: Simply press the "Get Form Button" above on this webpage to open our pdf file editor. There you'll find all that is required to work with your file.
Step 2: The editor offers the capability to change PDF forms in a range of ways. Change it by writing customized text, correct existing content, and include a signature - all within a few clicks!
It is an easy task to complete the document with this helpful guide! Here's what you should do:
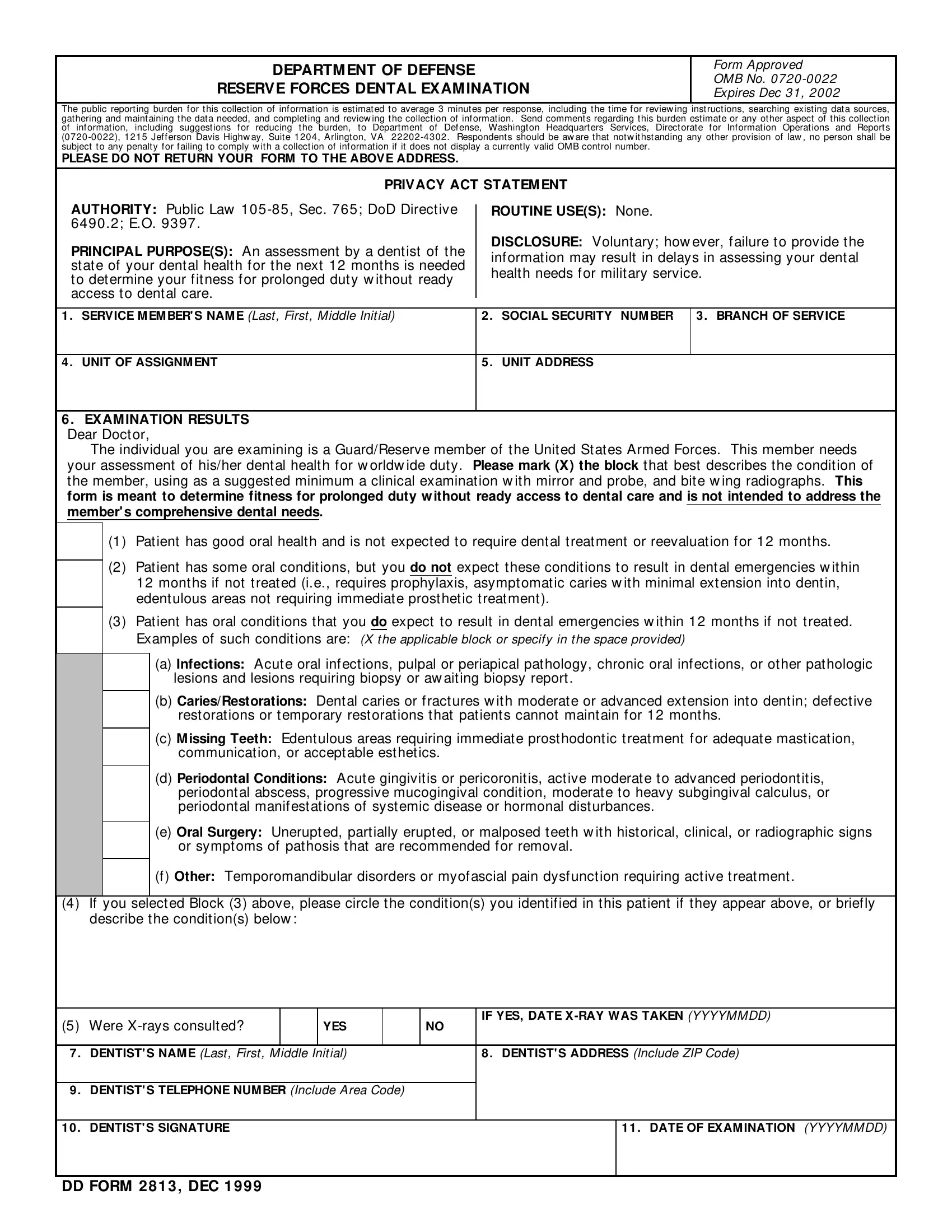
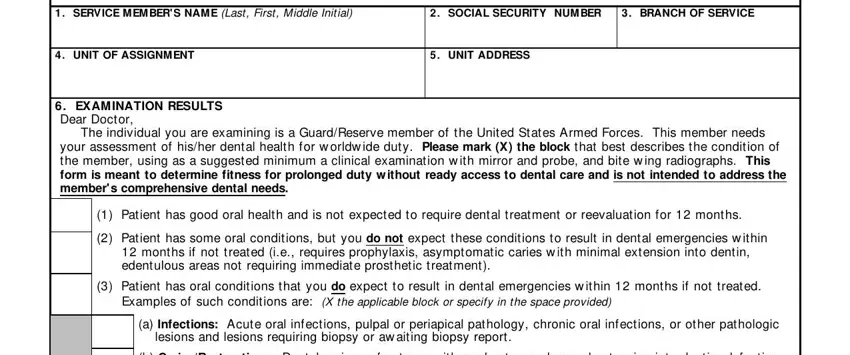
1. The DD Form 2813 fillable will require particular details to be inserted. Make certain the following blanks are finalized:
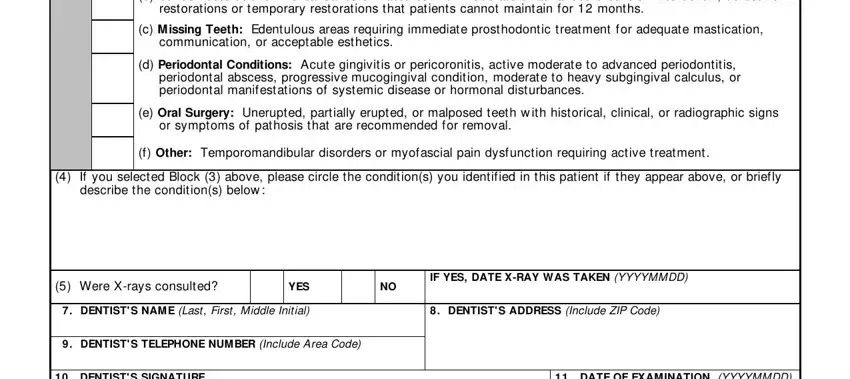
2. When the previous part is complete, you have to insert the required details in b CariesRestorations Dental caries, c M issing Teeth Edentulous areas, d Periodontal Conditions Acute, e Oral Surgery Unerupted partially, f Other Temporomandibular, If you selected Block above, Were Xrays consulted, YES, IF YES DATE XRAY WAS TAKEN YYYYMMDD, DENTIST S NAM E Last First Middle, DENTIST S ADDRESS Include ZIP Code, DENTIST S TELEPHONE NUM BER, DENTIST S SIGNATURE, and DATE OF EXAM INATION YYYYMMDD so you're able to progress further.
3. The next part is rather simple, DENTIST S SIGNATURE, DATE OF EXAM INATION YYYYMMDD, and DD FORM DEC - every one of these empty fields must be completed here.

In terms of DATE OF EXAM INATION YYYYMMDD and DD FORM DEC, ensure that you don't make any mistakes in this current part. Those two are the key ones in this PDF.
Step 3: Before moving on, ensure that form fields were filled in the correct way. Once you confirm that it's correct, click on “Done." After setting up a7-day free trial account at FormsPal, you will be able to download DD Form 2813 fillable or send it via email without delay. The file will also be available through your personal account menu with your every change. When using FormsPal, you can easily complete documents without having to worry about data leaks or data entries being distributed. Our protected software ensures that your personal information is maintained safely.