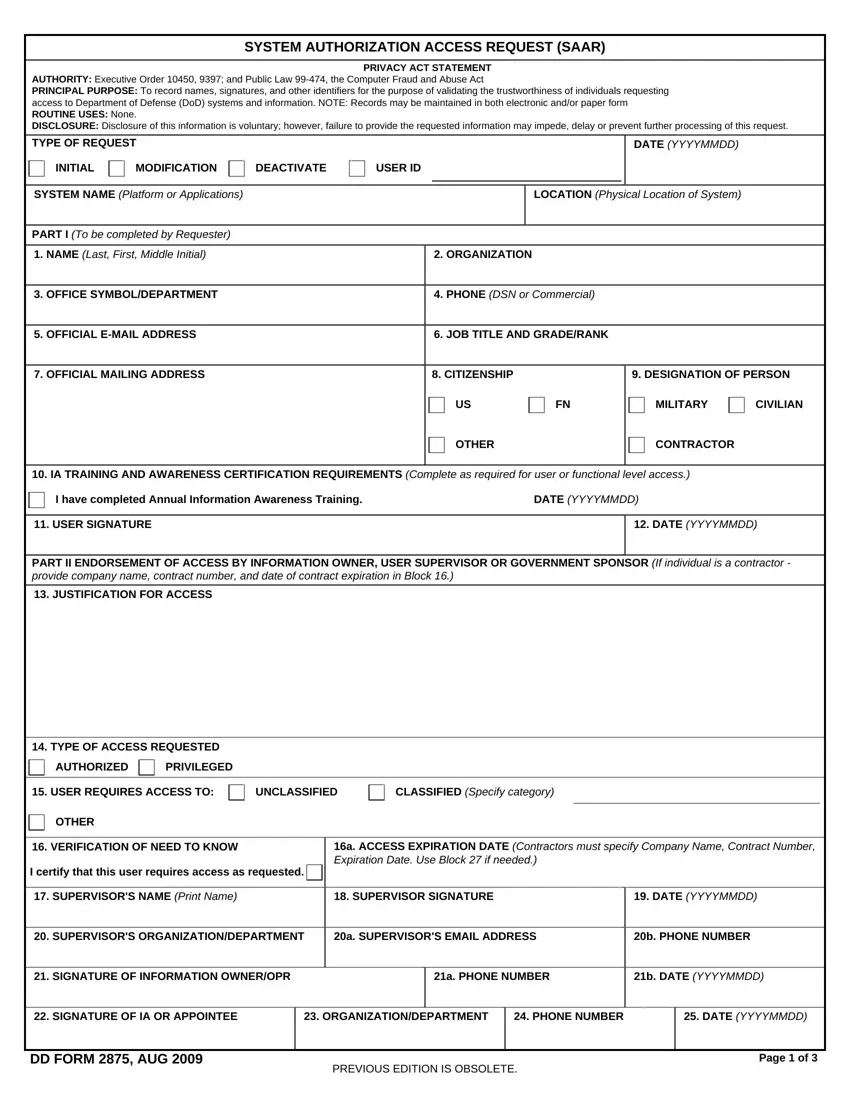
In an era where cybersecurity and controlled access are paramount within the Department of Defense (DoD), the DD Form 2875, or the System Authorization Access Request (SAAR), serves as a critical tool. This form not only standardizes the process for requesting access to DoD systems and information but also plays a vital role in validating the trustworthiness of individuals seeking such access. With its comprehensive structure, the form captures essential details like personal identification, job title, citizenship, level of access required, and information on required cybersecurity training. By mandating an endorsement process involving supervisors and Information Systems Security Officers (ISSOs), it ensures that access is granted based on a legitimate need to know, aligning with principles of least privilege and role-based access control. The form undergoes periodic updates, with the current version being valid until May 2025, underscoring the DoD's ongoing commitment to safeguarding sensitive information against unauthorized access. Thus, the DD Form 2875 embodies a proactive approach to information security, reflecting wider efforts within the military and affiliated civilian sectors to adapt to evolving cybersecurity challenges.
| Question | Answer |
|---|---|
| Form Name | Dd Form 2875 |
| Form Length | 3 pages |
| Fillable? | Yes |
| Fillable fields | 1 |
| Avg. time to fill out | 57 sec |
| Other names | dd form 2875, dd form 2875 fillable pdf, how to form saar, dd 2875 |
