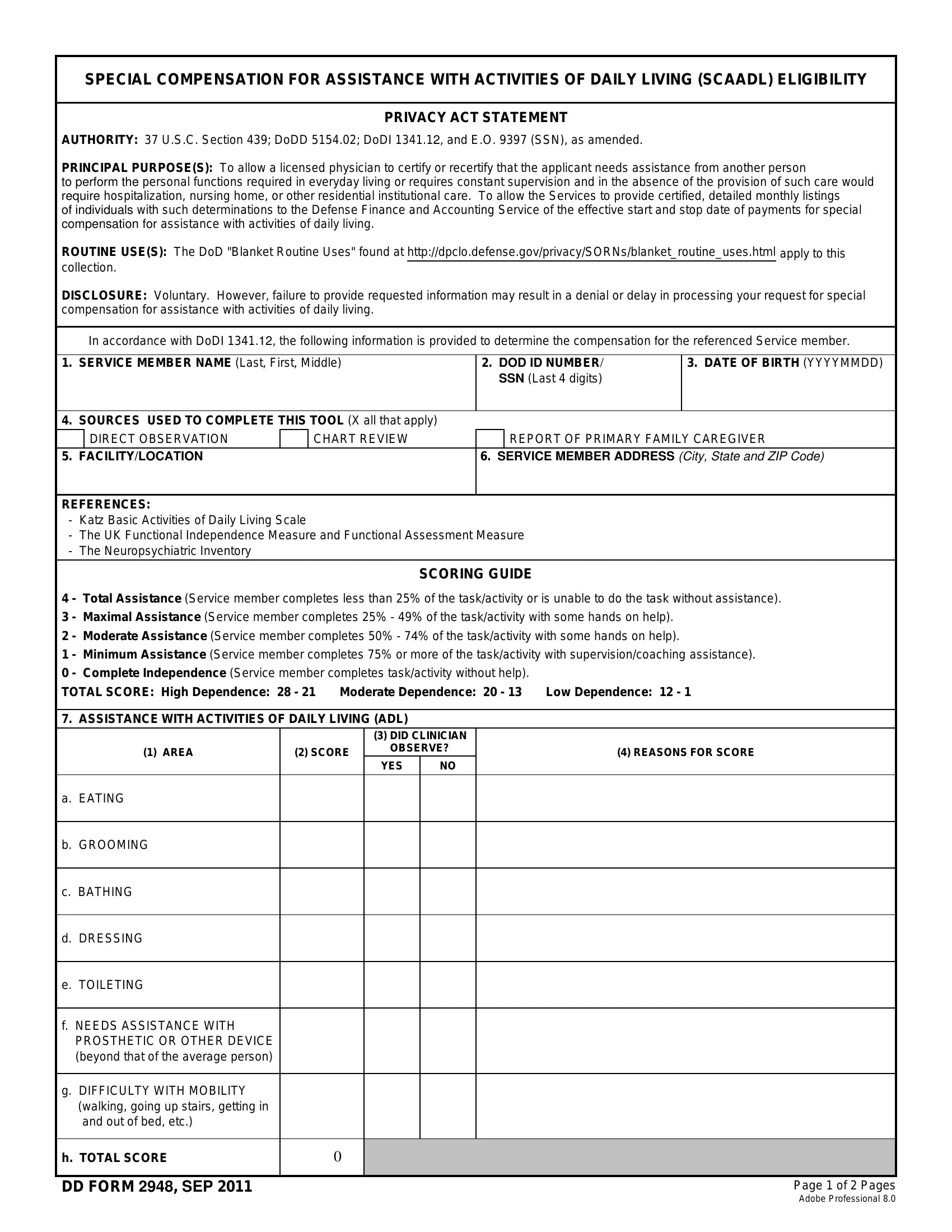
At the heart of providing care for those who have served lies the DD Form 2948, a document designed to assess and determine the level of Special Compensation for Assistance with Activities of Daily Living (SCAADL) for eligible service members. This important form is guided by authoritative legislation and directives, including 37 U.S.C. Section 439, DoDD 5154.02, and DoDI 1341.12, ensuring that the process adheres to a structured and legal framework. The principal purpose of the form is multifaceted: it allows a licensed physician to certify the need for caregiver assistance in daily living due to a service member's inability to perform personal functions or the requirement for constant supervision. Additionally, it outlines a system for calculating the compensation through a detailed scoring guide based on the Katz Basic Activities of Daily Living Scale, among other references. This assessment covers eating, grooming, bathing, mobility, and the need for supervision for safety reasons, providing a comprehensive look at the individual's requirements for caregiver support. With its intricate design, the form serves not only as a tool for assessment but also communicates the Defense Finance and Accounting Service (DFAS) role in processing the SCAADL compensation. It underscores the gravity of disclosing necessary information, a step that is voluntary, yet essential for rendering aid to those in need. Ultimately, the form embodies a critical process in acknowledging and supporting the profound needs of service members requiring caregiver assistance in their daily lives.
| Question | Answer |
|---|---|
| Form Name | Dd Form 2948 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | dd 2948, ICD-09, ADL, Katz |