
With the online PDF tool by FormsPal, it is easy to fill out or alter flight duties x here and now. Our tool is consistently developing to provide the best user experience possible, and that is thanks to our commitment to continuous improvement and listening closely to comments from customers. To get started on your journey, take these easy steps:
Step 1: Press the "Get Form" button at the top of this webpage to get into our tool.
Step 2: This editor provides the opportunity to modify nearly all PDF forms in a variety of ways. Modify it by writing your own text, adjust original content, and include a signature - all at your fingertips!
It is actually an easy task to complete the pdf using out helpful tutorial! Here is what you must do:
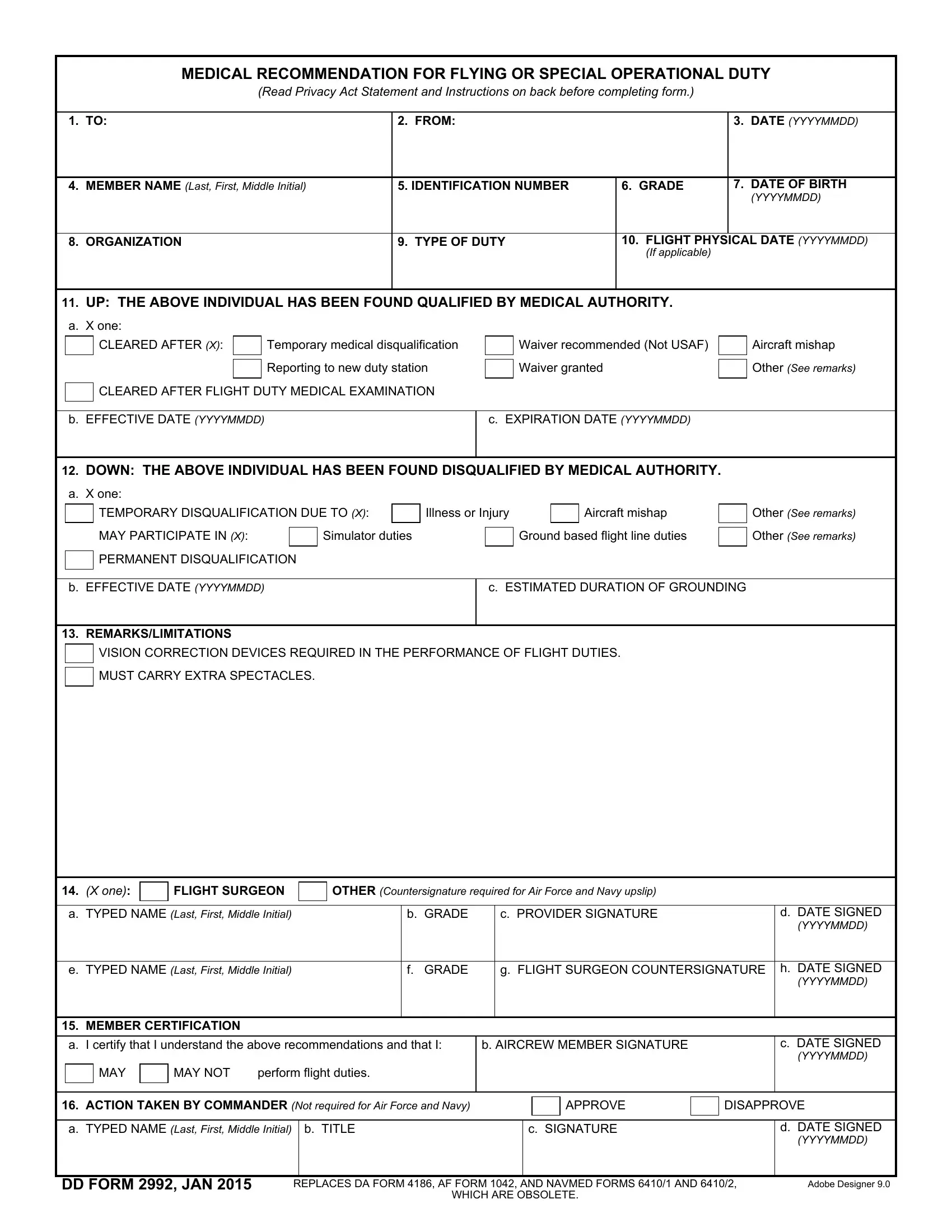
1. Fill out your flight duties x with a selection of essential blanks. Gather all of the necessary information and ensure nothing is forgotten!
2. Soon after filling in the previous part, head on to the next step and enter the necessary particulars in all these blanks - MAY PARTICIPATE IN X, Simulator duties, Ground based flight line duties, Other See remarks, PERMANENT DISQUALIFICATION, b EFFECTIVE DATE YYYYMMDD, c ESTIMATED DURATION OF GROUNDING, REMARKSLIMITATIONS, VISION CORRECTION DEVICES REQUIRED, MUST CARRY EXTRA SPECTACLES, X one, FLIGHT SURGEON, OTHER Countersignature required, a TYPED NAME Last First Middle, and b GRADE.
Be extremely careful when filling in Simulator duties and Ground based flight line duties, since this is the section where most users make some mistakes.
3. The following segment will be about e TYPED NAME Last First Middle, f GRADE, g FLIGHT SURGEON COUNTERSIGNATURE, MEMBER CERTIFICATION, a I certify that I understand the, b AIRCREW MEMBER SIGNATURE, MAY, MAY NOT, perform flight duties, h DATE SIGNED YYYYMMDD, c DATE SIGNED YYYYMMDD, ACTION TAKEN BY COMMANDER Not, APPROVE, DISAPPROVE, and a TYPED NAME Last First Middle - fill in each one of these blank fields.
Step 3: After rereading your form fields you have filled out, hit "Done" and you are all set! Get hold of your flight duties x after you subscribe to a 7-day free trial. Immediately get access to the pdf document in your FormsPal cabinet, along with any modifications and adjustments being all preserved! FormsPal guarantees secure document completion without personal data recording or any kind of sharing. Feel comfortable knowing that your details are in good hands here!