INSTRUCTIONS FOR COMPLETING THE
QUARTERLY CONTRIBUTION RETURN AND REPORT OF WAGES (CONTINUATION) (DE 9C)
PLEASE TYPE ALL INFORMATION
Did you know you can file this form online using the EDD’s e-Services for Business?
For a faster, easier, and more convenient method of reporting your DE 9C information, visit the EDD’s website at www.edd.ca.gov.
Contact the Taxpayer Assistance Center at (888) 745-3886 (voice) or TTY (800) 547-9565 (non-verbal) for additional forms or inquiries regarding
reporting wages or the subject status of employees. Refer to the California Employer’s Guide (DE 44) for additional information.
Please record information in the spaces provided. If you use a typewriter or printer, ignore the boxes and type in UPPER CASE as shown.
Do not use dollar signs, dashes, commas, or slashes ($ - , /).
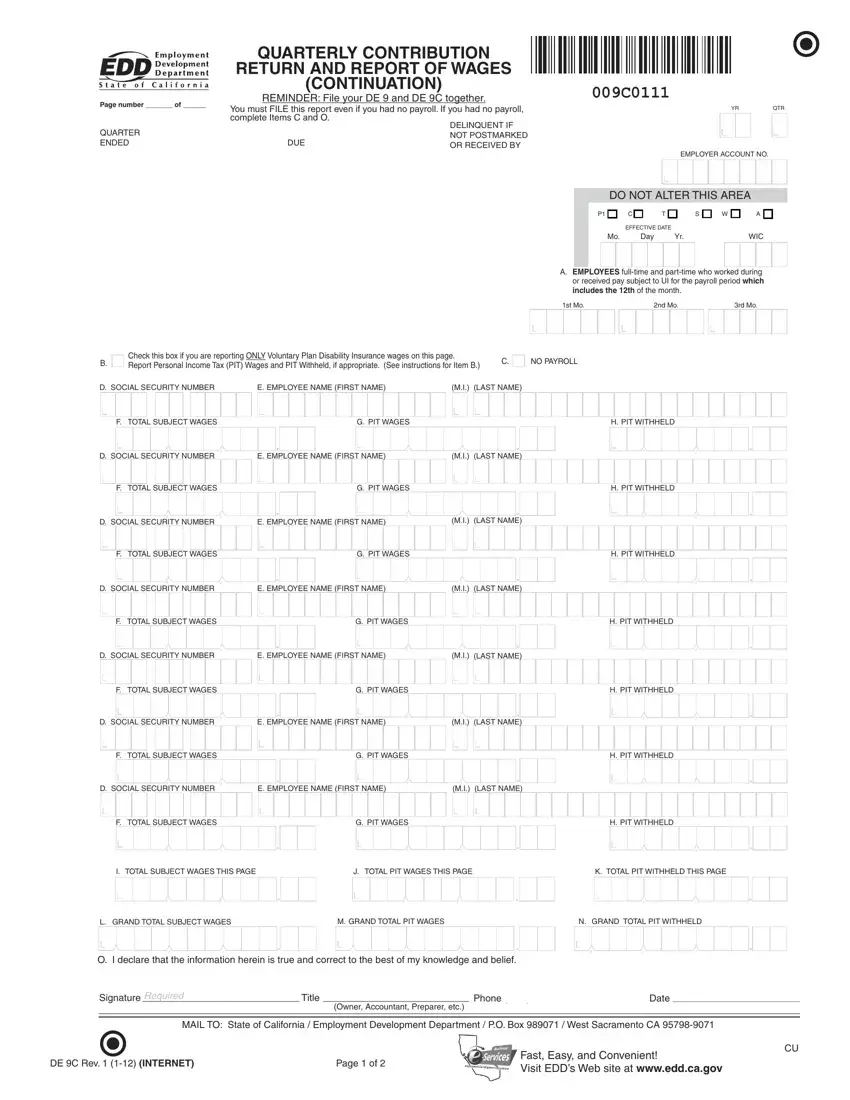
Retain a copy of the DE 9C form(s) for your records. If you have more than seven employees, use additional pages or a format approved by the Employment Development Department (EDD). If using more than one page, number the pages consecutively at the top of the form. If the form is not preprinted, enter your account number, business name and address, the year and quarter, and the quarter ended date. For information, specifications, and approvals of alternate forms, contact the Alternate Forms Coordinator at (916) 255-0649.
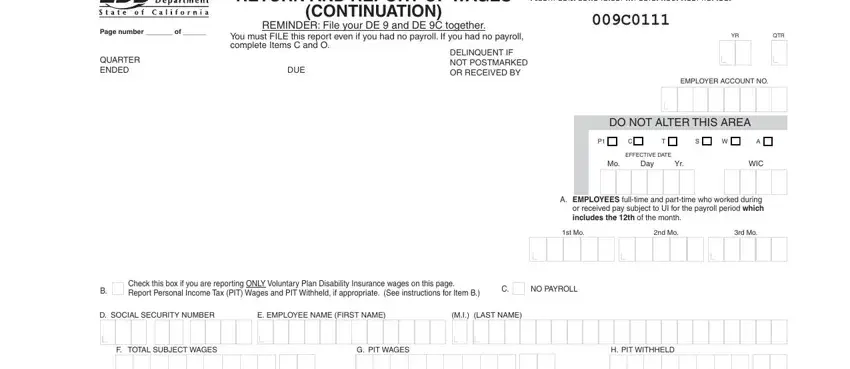
ITEM A. NUMBER OF EMPLOYEES: Page 1 only: Enter the number of full-time and part-time workers who worked during or received pay subject to Unemployment Insurance for the payroll period which includes the 12th day of the month. Please provide a count for each of the three months.
Blank fields will be identified as missing data.
ITEM B. Check this box ONLY if the employees reported are covered by an employer sponsored Voluntary Plan for the payment of disability benefits. If you also have employees covered under the State Plan for disability benefits, report their wages and withholdings separately on another page of the DE 9C.
WAGES AND WITHHOLDINGS TO REPORT ON A SEPARATE DE 9C
Prepare a DE 9C to report the types of exemptions listed below. All three exemptions can be reported on one DE 9C. Write the exemption title(s) at the top of the form (e.g., SOLE SHAREHOLDER), and report only those individuals under these categories. Report all other employees or individuals without exemptions on a separate
DE 9C.
•Religious Exemption: Employees who file and are approved by the EDD for an exemption from State Disability Insurance (SDI) taxes under Section 2902 of the California Unemployment Insurance Code (CUIC).
•Sole Shareholder: An individual who elects and is approved by the EDD to be excluded from SDI coverage for benefits and taxes under Section 637.1 of the CUIC.
•Third-Party Sick Pay: Recipients exempt from SDI taxes under Section 931.5 of the CUIC. Refer to the California Employer’s Guide (DE 44) for detailed instructions on how to report.
ITEM C. NO PAYROLL: Check this box if you had no payroll this quarter. Please sign and complete the information in Item O.
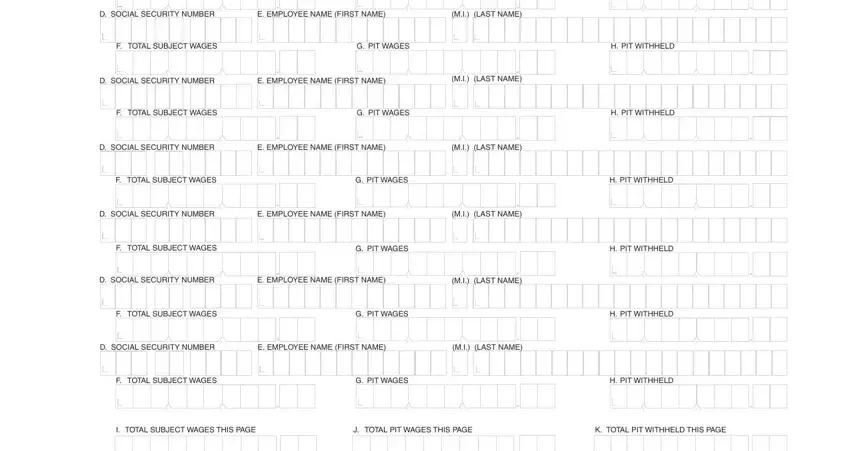
ITEM D. SOCIAL SECURITY NUMBER (SSN): Enter the SSN of each employee or individual to whom you paid wages in subject employment, paid Personal Income Tax (PIT) wages, and/or from whom you withheld PIT during the quarter. If someone does not have an SSN, report their name, wages, and/or withholdings without the SSN and TAKE IMMEDIATE STEPS TO SECURE ONE. Report the correct SSN to the EDD as soon as possible on a Quarterly Contribution and Wage Adjustment Form (DE 9ADJ).
ITEM E. EMPLOYEE NAME: Enter the name of each employee or individual to whom you paid wages in subject employment, paid PIT wages, and/or from whom you withheld PIT during the quarter.
ITEM F. TOTAL SUBJECT WAGES: Enter the total subject wages paid (including cents) to each employee during the quarter. Generally, most wages are considered “subject” wages. For special classes of employment and payments considered subject wages, refer to the California Employer’s Guide
(DE 44) under “Types of Employment” and “Types of Payments.”
ITEM G. PIT WAGES: Enter the amount of wages paid (including cents) that are subject to PIT, even if you do not withhold PIT from the
wages. You must enter PIT wages even if they are the same as total subject wages. For additional information regarding PIT wages, refer to the Information Sheet: Personal Income Tax Wages Reported on the Quarterly Contribution Return and Report of Wages (Continuation) (DE 9C) (DE 231PIT).
ITEM H. PIT WITHHELD: Enter the amount of PIT withheld from each individual during the quarter.
ITEM I. Enter the total subject wages paid (Item F) for each separate page. Do not carry this total forward from page to page.
ITEM J. Enter the total amount of PIT wages (Item G) for each separate page. Do not carry this total forward from page to page.
ITEM K. Enter the total PIT withheld (Item H) for each separate page. Do not carry this total forward from page to page.
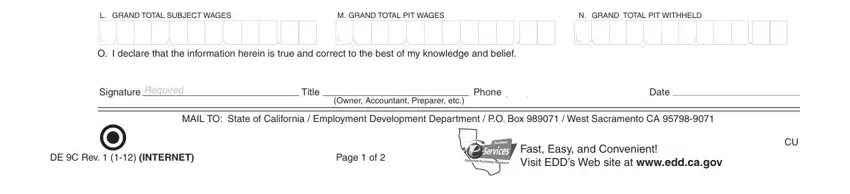
ITEM L. ON PAGE 1 or the last page, enter the grand total of total subject wages paid (Item I) for all pages for the quarter.*
ITEM M. ON PAGE 1 or the last page, enter the grand total of PIT wages (Item J) for all pages for the quarter.*
ITEM N. ON PAGE 1 or the last page, enter the grand total of PIT withheld (Item K) for all pages for the quarter.*
*NOTE: Provide separate grand totals for Voluntary Plan Disability Insurance reporting and special exemption reporting (Religious Exemption, Sole Shareholder, Third-Party Sick Pay). Combine all other Quarterly Contribution Return and Report of Wages (Continuation) (DE 9C)
pages to arrive at the grand totals for Items L, M, and N.
ITEM O. ON PAGE 1 ONLY, signature of preparer or responsible individual, including title, telephone number, and signature date.
 .
. .
.


 .
. .
.


 .
. .
.