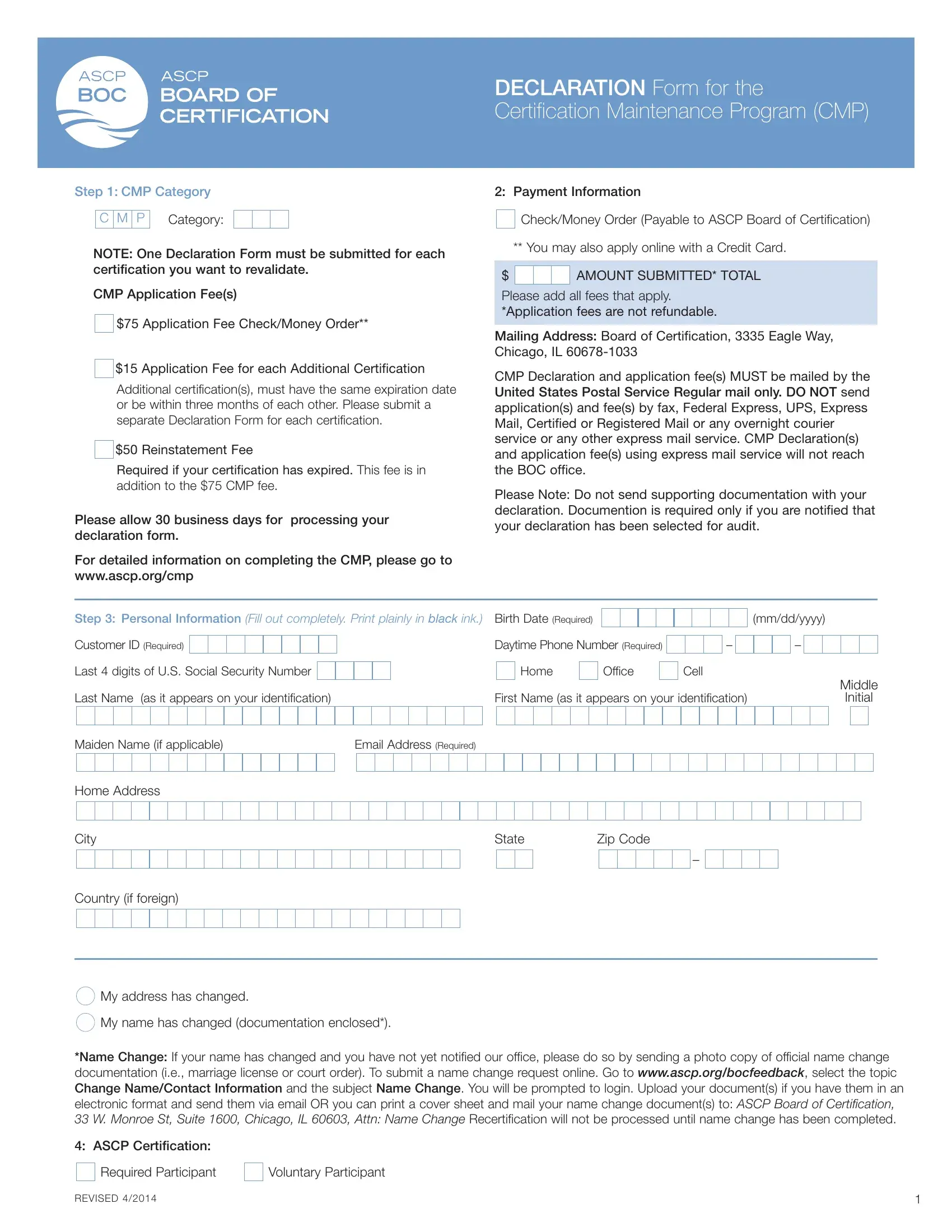
The Declaration Form for the Certification Maintenance Program is the official document required by the ASCP Board of Certification for credential holders revalidating their status. A separate form and payment are required for each individual certification being maintained.
Fee structure: a non-refundable $75 application fee applies per certification. If a credential has lapsed, a $50 reinstatement fee is added on top of the standard application fee. All fees are non-refundable once submitted.
Complete all personal and professional fields in black ink, writing legibly. Continuing education credits and qualifying professional activities must be recorded accurately for the maintenance period. Name changes require supporting documentation such as a marriage certificate or court order.
Submit the completed form exclusively via the United States Postal Service. The ASCP BOC does not process forms received by other means. Retain a copy of the completed form and payment receipt for your records. For related certification paperwork, see also the ACSI Certification Renewal Form.
| Question | Answer |
|---|---|
| Form Name | Declaration Cmp Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | certification cmp ascp, s service ascp, cmp declaration, mail ascp s |