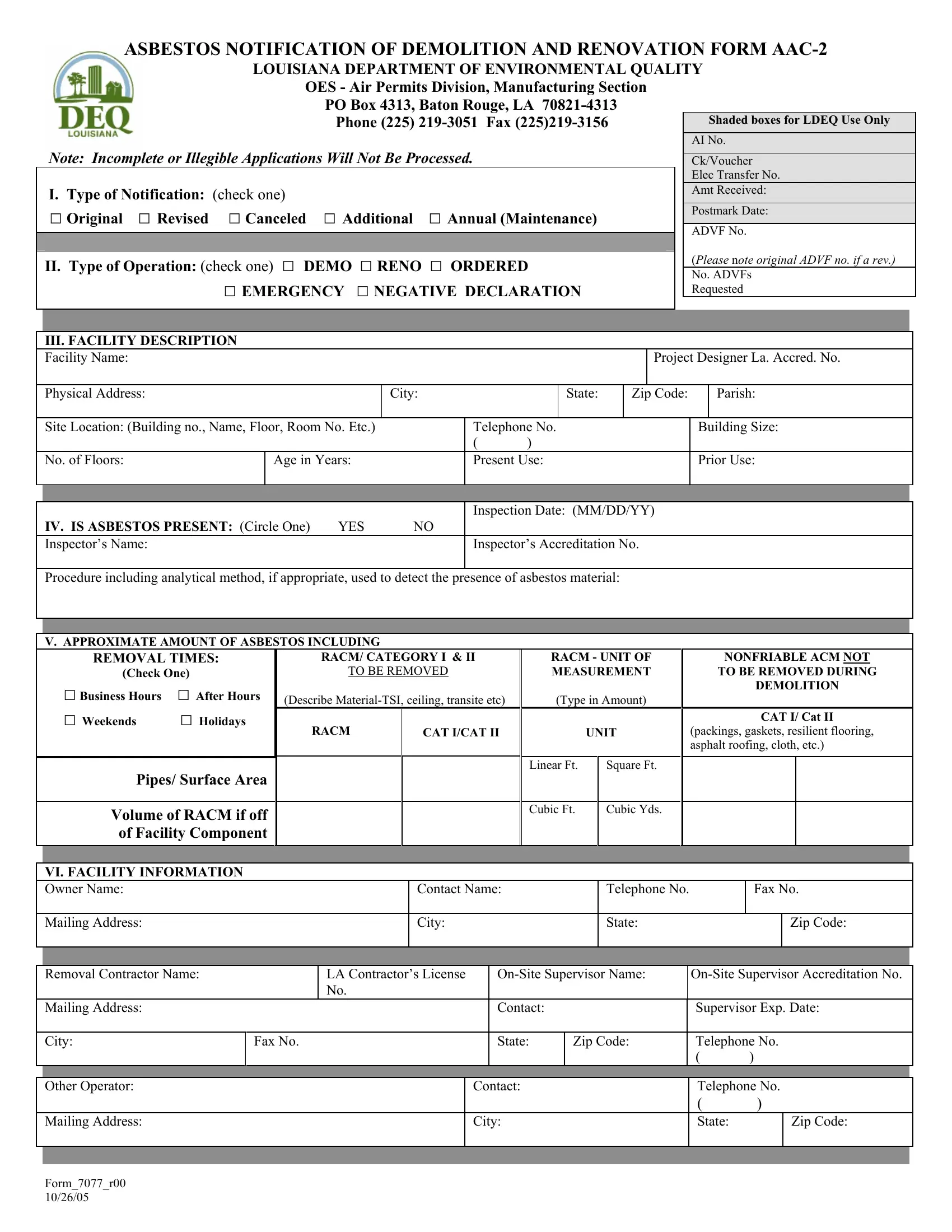
In the realm of occupational safety and environmental protection, meticulous procedures and documentation are paramount, especially when it comes to activities involving hazardous materials such as asbestos. The Deq Aac 2 form, formally known as the Asbestos Notification of Demolition and Renovation Form AAC-2, serves a critical role in this context. Managed by the Louisiana Department of Environmental Quality, specifically the OES - Air Permits Division, Manufacturing Section, this comprehensive document facilitates the communication of vital information regarding the demolition or renovation of facilities where asbestos is present. It meticulously outlines various aspects of the proposed activities, ranging from the type of operation, detailed facility description, asbestos presence, estimation of asbestos quantities, to the information about the facility owner, the removal contractor, waste transporter, and disposal site. Furthermore, it delves into scheduled dates for asbestos removal and subsequent demolition or renovation, addresses procedures for emergency renovations, and sets forth certification requirements for the individuals involved in these operations. The form's elaborate structure ensures that all necessary precautions are taken to prevent asbestos exposure, thereby safeguarding public health and safety and preserving environmental quality. The completion and submission process, underscored by specific notification fees and deadlines, underscores the Louisiana Department of Environmental Quality's stringent oversight and commitment to enforcing regulatory compliance in asbestos management.
| Question | Answer |
|---|---|
| Form Name | Deq Form Aac 2 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | r00, LOUISIANA, YY, OES |
