
The PDF editor makes it easy to manage the dfeh form document. You will be able to generate the document right away by using these basic steps.
Step 1: Get the button "Get Form Here" and select it.
Step 2: It's now possible to alter the dfeh form. This multifunctional toolbar will allow you to add, eliminate, change, and highlight content material or perhaps carry out many other commands.
Provide the details requested by the program to prepare the file.
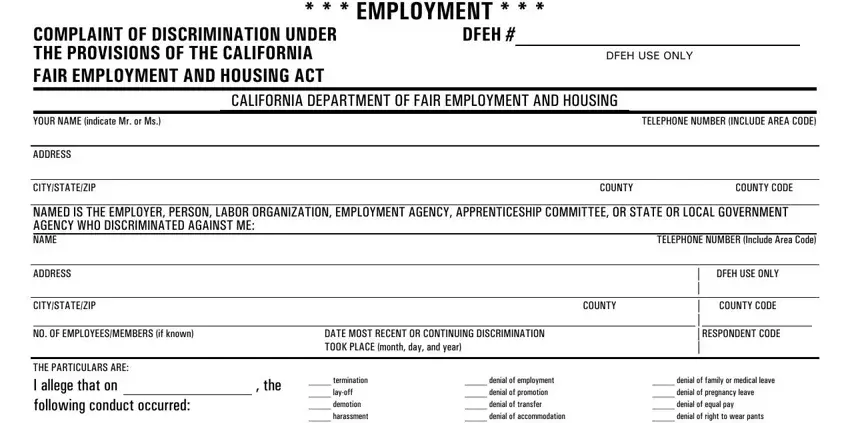
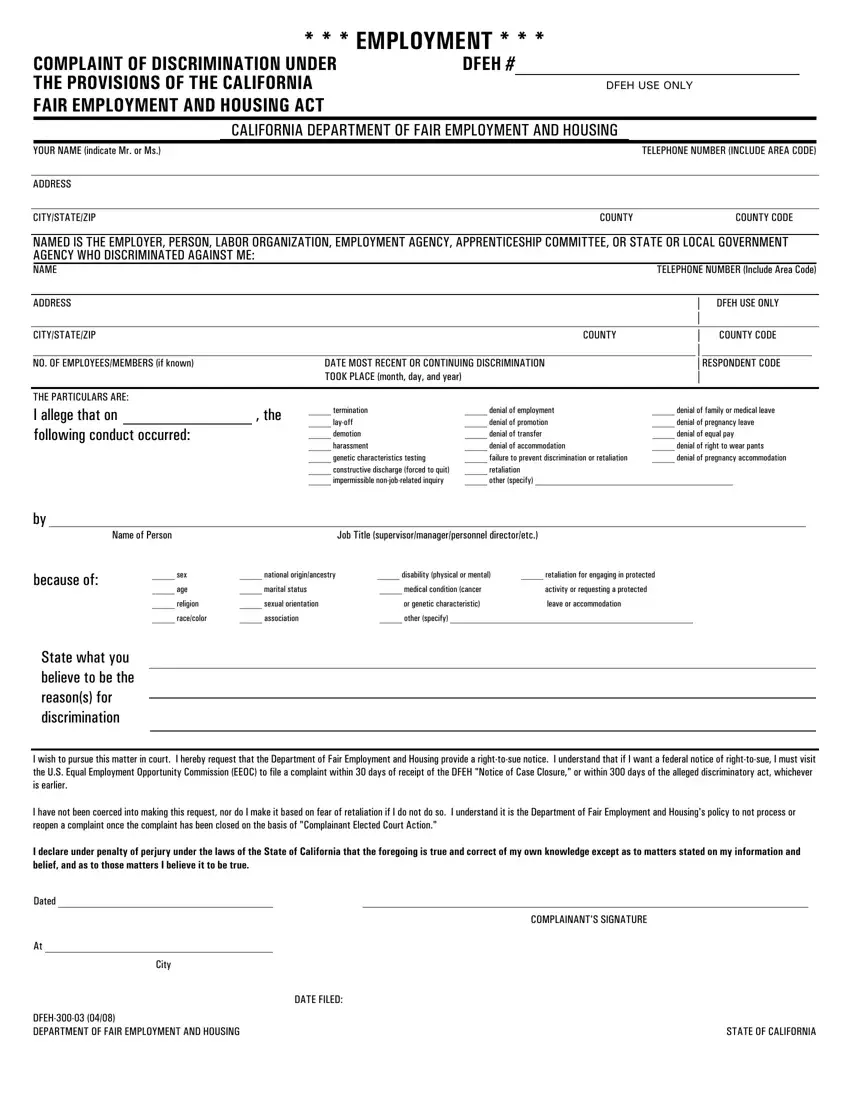
Fill in the termination layoff demotion, denial of employment denial of, denial of family or medical leave, Name of Person, Job Title, because of, sex, age, national originancestry, disability physical or mental, retaliation for engaging in, marital status, medical condition cancer, activity or requesting a protected, and religion fields with any information that will be asked by the platform.
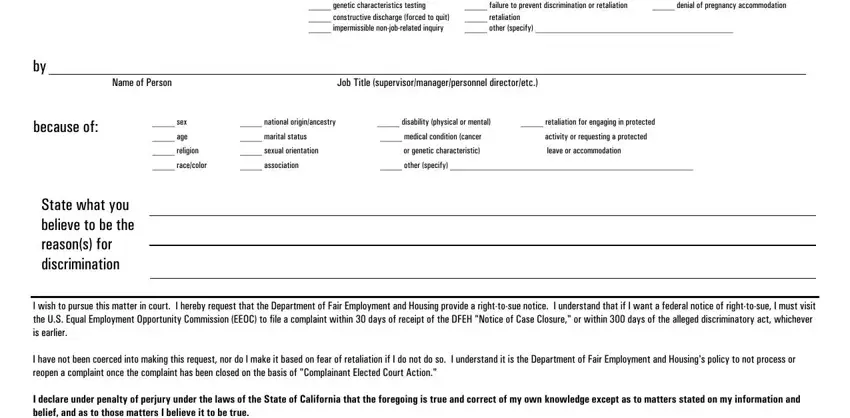
You'll have to provide certain data within the segment I declare under penalty of perjury, Dated, City, COMPLAINANTS SIGNATURE, DFEH DEPARTMENT OF FAIR, DATE FILED, and STATE OF CALIFORNIA.
You need to describe the rights and responsibilities of both parties in section YOUR RACEETHNICITY Check one, YOUR PRIMARY LANGUAGE specify, YOUR AGE, IF FILING BECAUSE OF YOUR NATIONAL, YOUR OCCUPATION Clerical Craft, and HOW YOU HEARD ABOUT DFEH Attorney.
Finish the form by taking a look at these particular sections: IF FILING BECAUSE OF YOUR NATIONAL, IF FILING BECAUSE OF MARITAL, IF FILING BECAUSE OF RELIGION YOUR, IF FILING BECAUSE OF SEX THE, HOW YOU HEARD ABOUT DFEH Attorney, DO YOU HAVE AN ATTORNEY WHO HAS, Yes No, PLEASE PROVIDE YOUR ATTORNEYS NAME, DFEH Department of Fair, and Your Signature Date.
Step 3: Click "Done". Now you may transfer the PDF form.
Step 4: In avoiding probable future problems, you should obtain a minimum of two duplicates of every single document.
