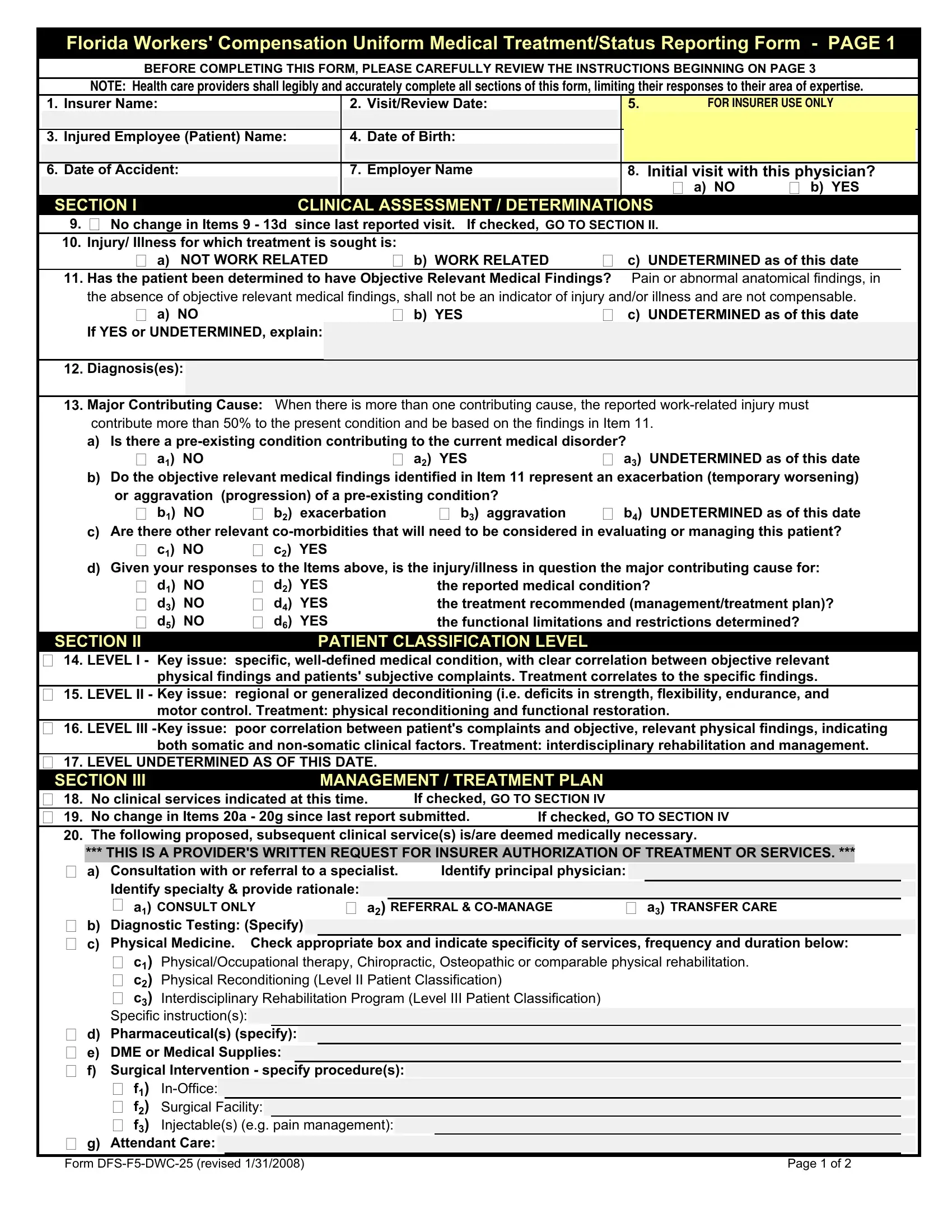
In the realm of workers' compensation in Florida, the DFS F5 DWC 25 form stands as a pivotal document, designed to streamline communication between healthcare providers, insurers, and employers regarding the medical treatment and status of injured employees. This comprehensive form, officially titled Florida Workers' Compensation Uniform Medical Treatment/Status Reporting Form, serves multiple critical functions. It captures the insurer's details, the dates of medical visits or reviews, and the injured employee’s personal and accident-related information. Health care providers are required to complete this form with legible accuracy, ensuring that their responses are confined to their areas of expertise. The form encompasses several sections, including clinical assessments/determinations on the work-relatedness of the injury, objective relevant medical findings, major contributing cause of the condition, and the patient's classification level based on the severity and nature of their condition. Furthermore, it outlines a management or treatment plan, delineates any functional limitations or restrictions, and, when applicable, establishes the date of maximum medical improvement and assigns a permanent impairment rating. The instructions for completing the DFS F5 DWC 25 form emphasize its role in the authorization of treatment services, making it an indispensable tool in the administration of workers' compensation claims in Florida. As such, it embodies a comprehensive approach to documenting and managing the care of injured workers, ensuring their treatment is accurately reflected and communicated to all pertinent parties.
| Question | Answer |
|---|---|
| Form Name | Dfs F5 Dwc 25 Form |
| Form Length | 18 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 4 min 30 sec |
| Other names | f5dwc, dwc25, dwc 25 form 2021, dwc 25 form florida |
