
This guide provides a step-by-step approach to filling out the DHHS Incident Report Form to ensure compliance and effective communication of incident details.
1. Identify the Type of Incident
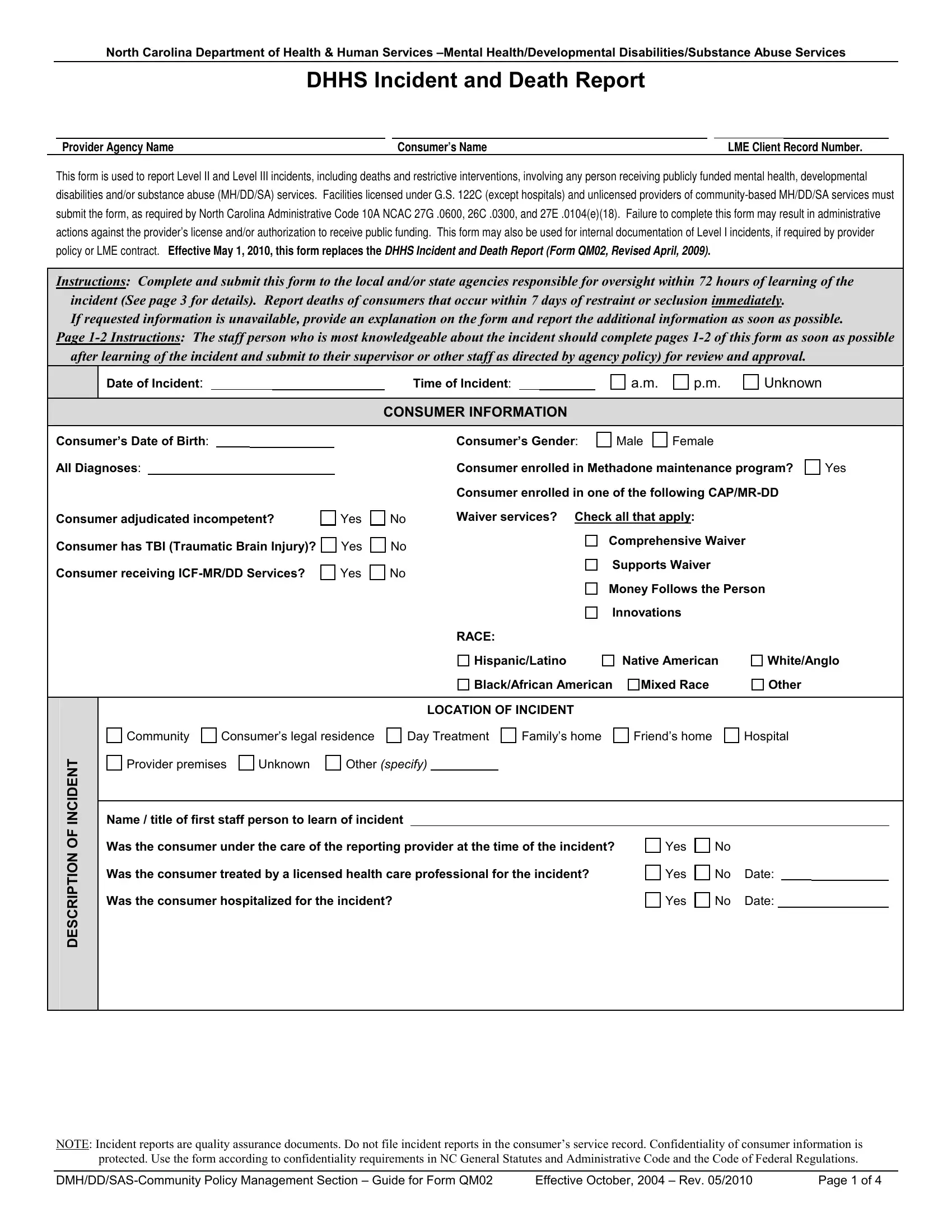
Determine the level of the incident (Level II or Level III) you are reporting. Level II incidents are moderate in severity, while Level III incidents are more severe, including deaths and situations needing immediate reporting.
2. Fill in Provider and Consumer Information
Enter the provider agency name, consumer's name, and the Local Management Entity (LME) client record number at the top of the form.
3. Document Incident Details
Record the date and time of the incident as accurately as possible. Under the description section, briefly describe the incident, including who was involved, what happened, when and where it occurred, and how it unfolded.
4. Complete Consumer Information Section
Provide detailed information about the consumer involved, including date of birth, diagnoses, and other pertinent details, such as whether the consumer has a traumatic brain injury (TBI) or is receiving specific services like Methadone maintenance or CAP/MR-DD Waiver services.
5. Report Any Restrictive Interventions Used
If any restrictive interventions such as physical restraint, isolation, or seclusion were used during the incident, document this. Specify whether the intervention is part of the consumer's Individual Service Plan and if it was administered appropriately.
6. Specify the Location and Nature of the Incident
Indicate where the incident occurred (e.g., community, provider premises, consumer's legal residence) and check the applicable type of incident from the options provided, such as injury, abuse allegation, medication error, or consumer behavior.
7. Attach Supporting Documents
If there are additional reports or documentation related to the incident, such as a Restrictive Intervention Details Report (Form QM03), attach these to the form.
8. Review and Approve the Form
The staff member most knowledgeable about the incident should fill out the form initially. After completion, a supervisor or designated staff member should review and approve it to ensure all information is accurate and complete before submission.
9. Submit the Form
Submit the completed form to the appropriate local and/or state oversight agencies within the required time frames.