
the dhmh 4345 form can be completed online very easily. Simply open FormsPal PDF tool to complete the task promptly. Our professional team is ceaselessly working to expand the editor and ensure it is even easier for users with its extensive features. Unlock an endlessly progressive experience now - take a look at and uncover new possibilities as you go! All it requires is several basic steps:
Step 1: First, open the tool by clicking the "Get Form Button" above on this site.
Step 2: Using this state-of-the-art PDF editor, it is easy to do more than just fill out forms. Express yourself and make your documents seem faultless with customized text incorporated, or tweak the file's original content to perfection - all that backed up by the capability to add just about any pictures and sign it off.
If you want to fill out this PDF document, ensure that you type in the right details in each and every blank field:
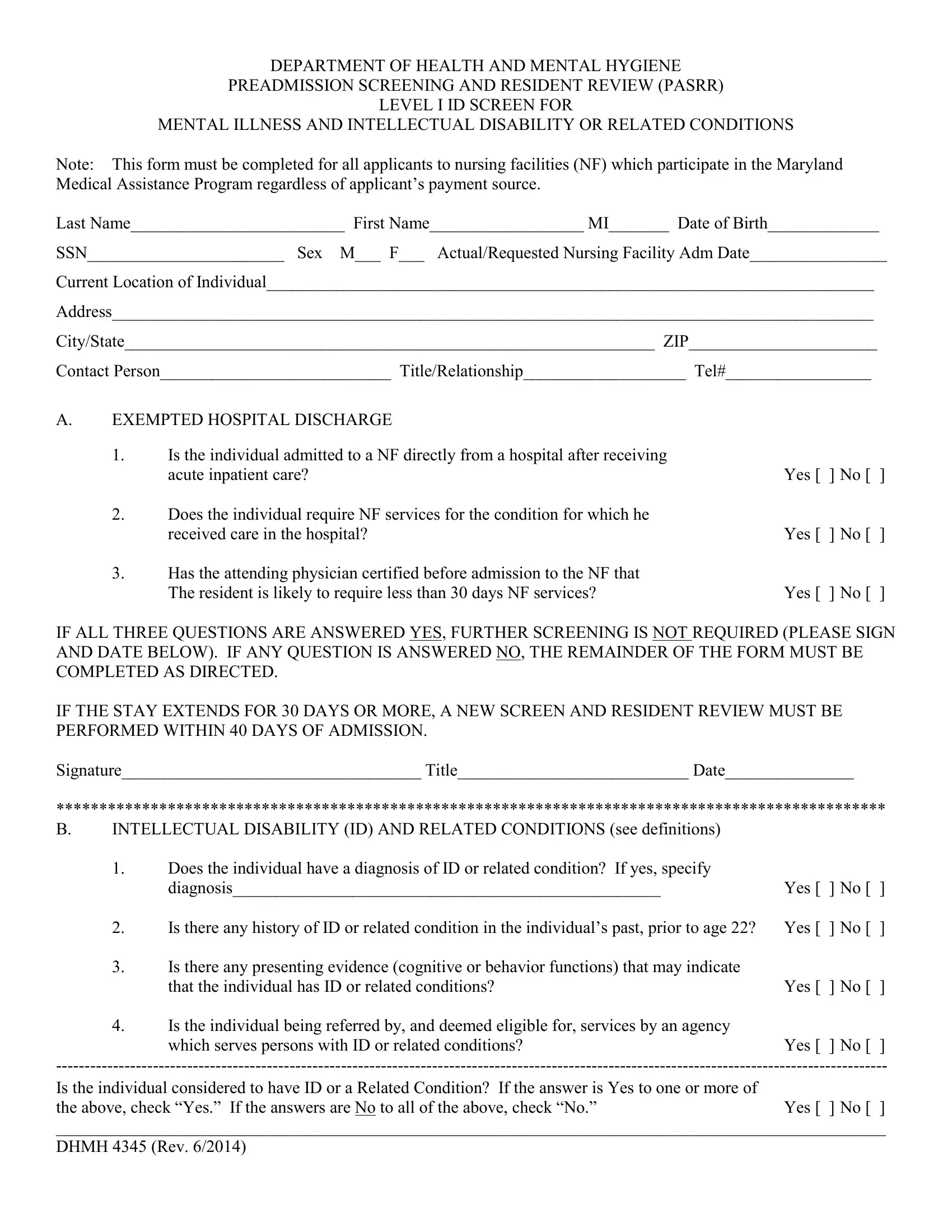
1. The the dhmh 4345 form usually requires particular information to be typed in. Be sure the following blank fields are filled out:
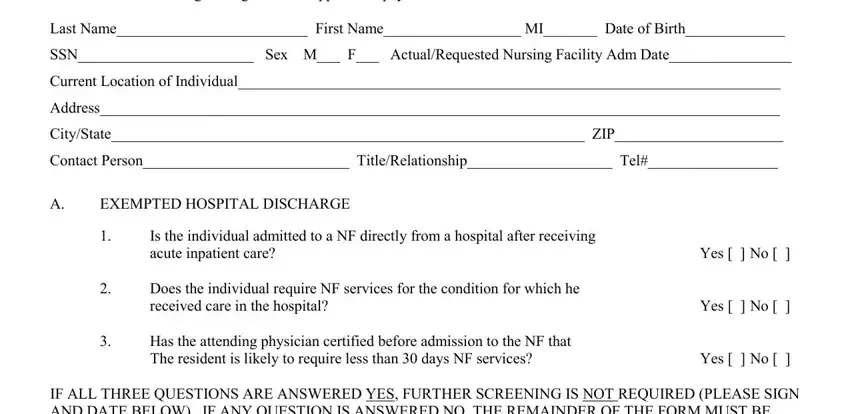
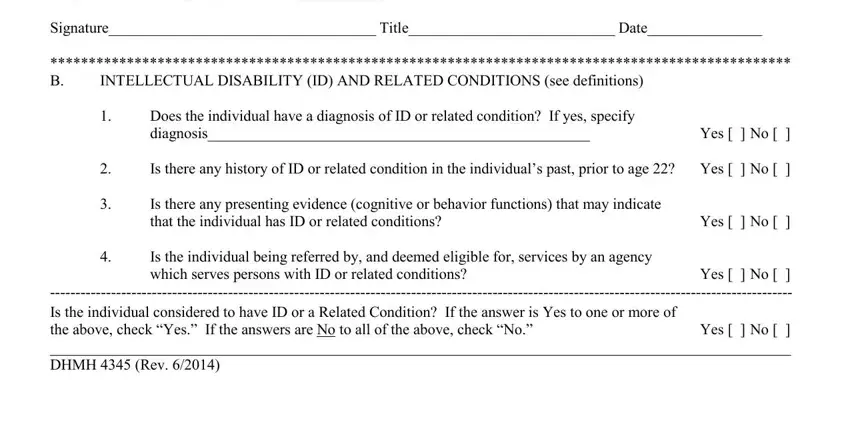
2. Soon after this section is filled out, proceed to enter the applicable information in all these - IF ALL THREE QUESTIONS ARE, Is there any presenting evidence, Is the individual being referred, Does the individual have a, Is there any history of ID or, INTELLECTUAL DISABILITY ID AND, Yes No, and Yes No.
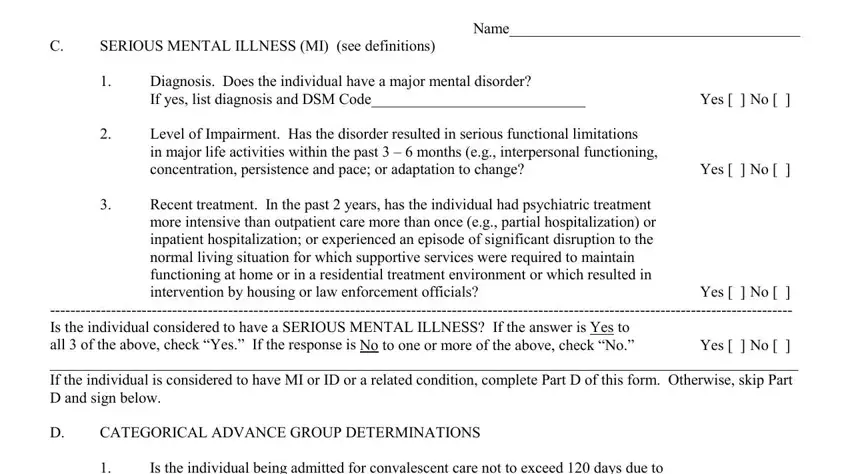
3. Completing Name, Yes No, Yes No, Yes No, SERIOUS MENTAL ILLNESS MI see, CATEGORICAL ADVANCE GROUP, Diagnosis Does the individual have, Level of Impairment Has the, Is the individual being admitted, Recent treatment In the past, and C Yes No Is the individual is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
People often make errors while filling out Name in this area. Ensure that you go over whatever you type in right here.
4. This next section requires some additional information. Ensure you complete all the necessary fields - Is the individual being admitted, C Yes No Is the individual, Does the individual have a severe, Is this individual being, Is the individual being admitted, Does the individual have a, Yes No, Yes No, Yes No, and Yes No - to proceed further in your process!
5. This final notch to complete this form is integral. Ensure that you fill in the mandatory form fields, including C Yes No Is the individual, prior to submitting. If you don't, it could produce an unfinished and potentially unacceptable paper!

Step 3: Immediately after rereading your fields, hit "Done" and you are all set! Get hold of the the dhmh 4345 form as soon as you join for a free trial. Easily view the form from your personal account page, together with any edits and changes being all preserved! FormsPal provides safe document completion without personal data recording or distributing. Feel safe knowing that your details are safe here!