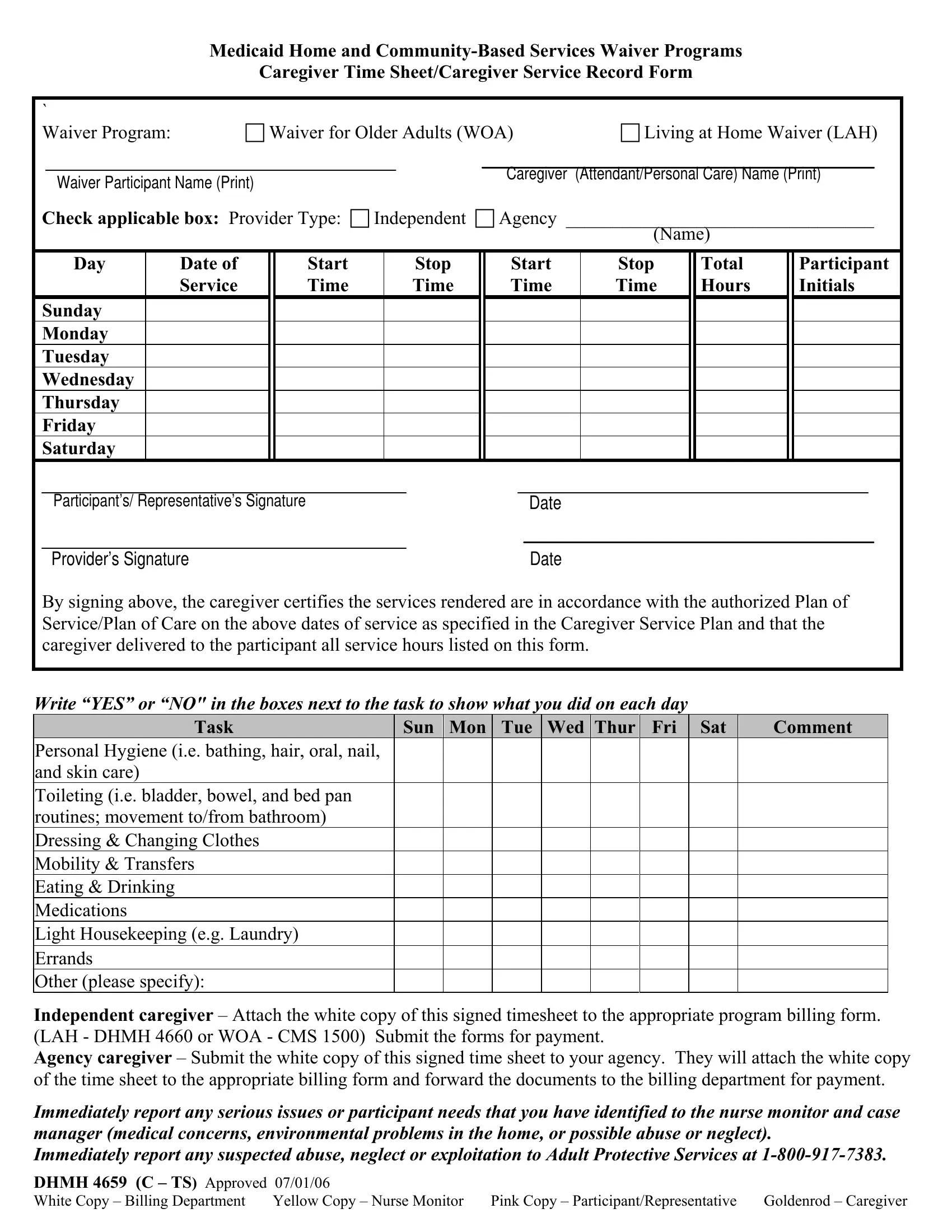
At the heart of providing targeted, personalized care under Medicaid Home and Community-Based Services Waiver Programs lies the essential documentation requirement fulfilled by the DHMH 4659 form. This detailed Caregiver Time Sheet/Caregiver Service Record serves as a critical record that bridges the communication between caregivers, participants, and administrative bodies overseeing caregiving services. It applies to specific waivers, notably the Waiver for Older Adults (WOA) and the Living at Home Waiver (LAH), ensuring that elderly participants receive the support they need to live an independent and dignified life at home. The form captures daily caregiving activities ranging from personal hygiene to medication management, and it meticulously records the start and stop times of service each day. By initialing their service hours, caregivers confirm that their assistance aligns with the participant's authorized Plan of Service/Plan of Care. This process not only ensures accountability but also fosters transparency by requiring signatures from both the caregiver and the participant or their representative. Importantly, it guides caregivers on the correct procedure for submitting their recorded hours for payment, differentiating between independent and agency caregivers. Furthermore, it underscores the imperative of reporting any serious issues, including potential abuse, neglect, or exploitation, thereby prioritizing participant safety and well-being. The distribution of form copies serves as an organized method to keep all involved parties informed, making the DHMH 4659 form a cornerstone of efficient caregiving within Medicaid's waiver programs.
| Question | Answer |
|---|---|
| Form Name | Dhmh 4659 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | DHMH4659_C TS woa dhmh form |
Medicaid Home and
Caregiver Time Sheet/Caregiver Service Record Form
` |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Waiver Program: |
|
Waiver for Older Adults (WOA) |
|
Living at Home Waiver (LAH) |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Caregiver |
(Attendant/Personal Care) Name (Print) |
|||||||||
|
|
Waiver Participant Name (Print) |
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Check applicable box: Provider Type: |
Independent |
|
Agency _________________________________ |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Name) |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Day |
|
Date of |
|
Start |
|
|
|
Stop |
|
Start |
|
Stop |
|
Total |
|
Participant |
||||
|
|
|
|
Service |
|
Time |
|
|
|
Time |
|
Time |
|
Time |
|
Hours |
|
Initials |
||||
|
Sunday |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Monday |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Tuesday |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Wednesday |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Thursday |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Friday |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Saturday |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Participant’s/ Representative’s Signature |
|
|
|
|
|
|
|
Date |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Provider’s Signature |
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
|
|
|
||
By signing above, the caregiver certifies the services rendered are in accordance with the authorized Plan of Service/Plan of Care on the above dates of service as specified in the Caregiver Service Plan and that the caregiver delivered to the participant all service hours listed on this form.
Write “YES” or “NO" in the boxes next to the task to show what you did on each day
Task |
Sun |
Mon |
Tue |
Wed |
Thur |
Fri |
Sat |
Comment |
Personal Hygiene (i.e. bathing, hair, oral, nail, and skin care)
Toileting (i.e. bladder, bowel, and bed pan routines; movement to/from bathroom)
Dressing & Changing Clothes
Mobility & Transfers
Eating & Drinking
Medications
Light Housekeeping (e.g. Laundry)
Errands
Other (please specify):
Independent caregiver – Attach the white copy of this signed timesheet to the appropriate program billing form. (LAH - DHMH 4660 or WOA - CMS 1500) Submit the forms for payment.
Agency caregiver – Submit the white copy of this signed time sheet to your agency. They will attach the white copy of the time sheet to the appropriate billing form and forward the documents to the billing department for payment.
Immediately report any serious issues or participant needs that you have identified to the nurse monitor and case manager (medical concerns, environmental problems in the home, or possible abuse or neglect).
Immediately report any suspected abuse, neglect or exploitation to Adult Protective Services at
DHMH 4659 (C – TS) Approved 07/01/06 |
|
|
|
White Copy – Billing Department |
Yellow Copy – Nurse Monitor |
Pink Copy – Participant/Representative |
Goldenrod – Caregiver |