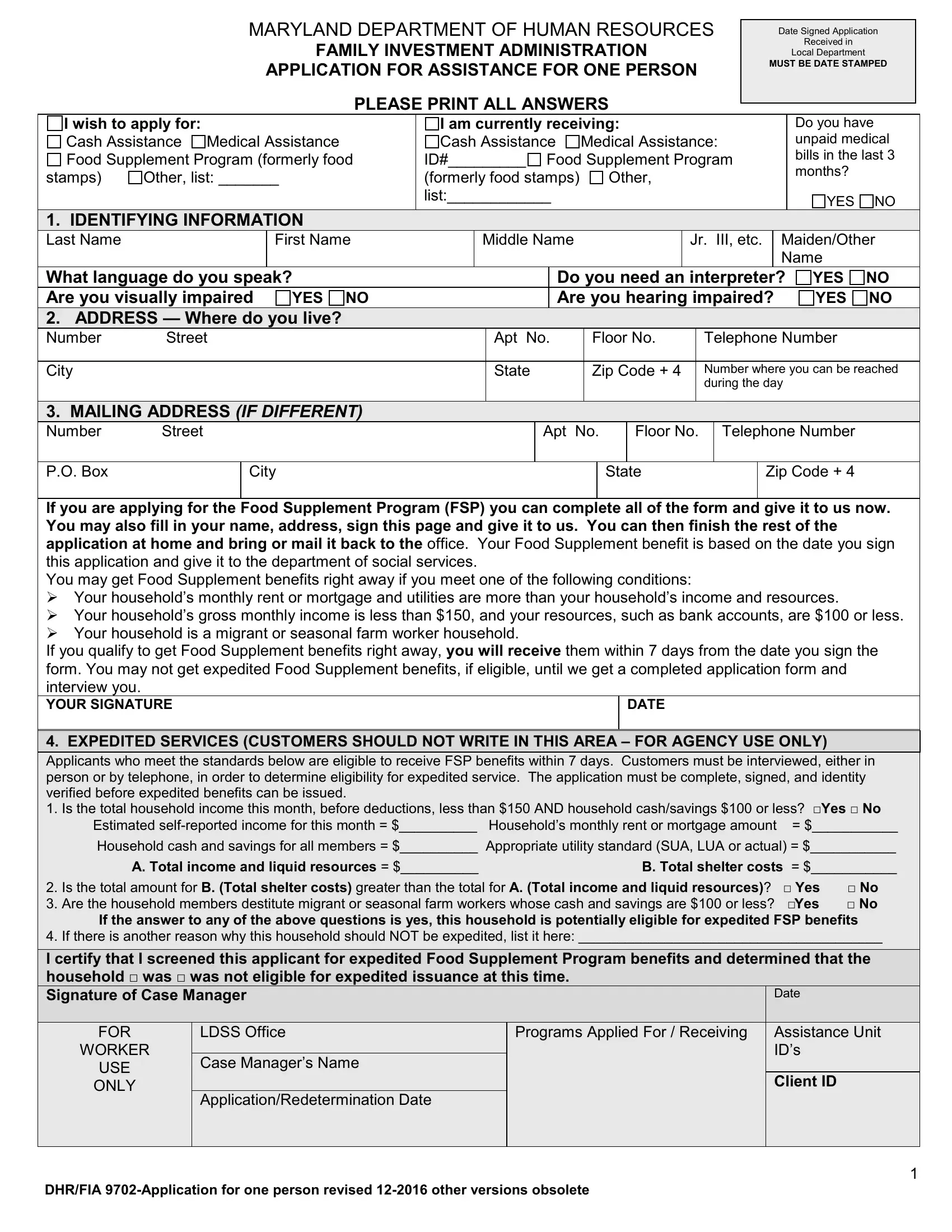
Navigating through the complexities of applying for assistance can often feel overwhelming, but understanding the essentials of forms like the Maryland Department of Human Resources Family Investment Administration Application for Assistance, or as it's formally known, the DHR 9702 form, is a crucial first step. Designed specifically for individuals seeking support, this comprehensive document covers a spectrum of assistance programs including Cash Assistance, Medical Assistance, and the Food Supplement Program, formerly known as food stamps. Required to be date-stamped upon receipt, the form serves as a crucial element in the process, marking the beginning of the applicant's journey towards obtaining necessary aid. Applicants must clearly detail personal information, current assistance received, and whether they have unpaid medical bills, among other specifics. The form also addresses the expedited services for those in immediate need, highlighting the state's commitment to acting swiftly under certain conditions. By demystifying the DHR 9702 form, individuals can more confidently navigate their way through the application process, understanding each section's relevance to their unique circumstances and the broader context of state-supported assistance programs.
| Question | Answer |
|---|---|
| Form Name | Dhr 9702 Form |
| Form Length | 14 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min 30 sec |
| Other names | md dhr application assistance one, dhr fia 9702 one, md dhr fia, dhs fia 9702 |
MARYLAND DEPARTMENT OF HUMAN RESOURCES
FAMILY INVESTMENT ADMINISTRATION
APPLICATION FOR ASSISTANCE FOR ONE PERSON
PLEASE PRINT ALL ANSWERS
Date Signed Application
Received in
Local Department
MUST BE DATE STAMPED
I wish to apply for:
Cash Assistance Medical Assistance Food Supplement Program (formerly food
stamps) |
Other, list: _______ |
I am currently receiving:
Cash Assistance |
Medical Assistance: |
ID#_________ Food Supplement Program |
|
(formerly food stamps) |
Other, |
list:____________ |
|
Do you have unpaid medical bills in the last 3 months?
YES NO
1. IDENTIFYING INFORMATION
Last Name
First Name
Middle Name
Jr. III, etc.
Maiden/Other Name
What language do you speak? |
|
|
Do you need an interpreter? |
YES |
NO |
||||
Are you visually impaired |
YES NO |
|
|
Are you hearing impaired? |
YES |
NO |
|||
2. ADDRESS — Where do you live? |
|
|
|
|
|
|
|
||
Number |
Street |
|
Apt No. |
|
Floor No. |
Telephone Number |
|
||
|
|
|
|
|
|
|
|||
City |
|
|
State |
|
Zip Code + 4 |
Number where you can be reached |
|||
|
|
|
|
|
|
|
during the day |
|
|
|
|
|
|
|
|
|
|
||
3. MAILING ADDRESS (IF DIFFERENT) |
|
|
|
|
|
|
|
||
Number Street
Apt No.
Floor No.
Telephone Number
P.O. Box
City
State
Zip Code + 4
If you are applying for the Food Supplement Program (FSP) you can complete all of the form and give it to us now. You may also fill in your name, address, sign this page and give it to us. You can then finish the rest of the application at home and bring or mail it back to the office. Your Food Supplement benefit is based on the date you sign this application and give it to the department of social services.
You may get Food Supplement benefits right away if you meet one of the following conditions:
Your household’s monthly rent or mortgage and utilities are more than your household’s income and resources.
Your household’s gross monthly income is less than $150, and your resources, such as bank accounts, are $100 or less.
Your household is a migrant or seasonal farm worker household.
If you qualify to get Food Supplement benefits right away, you will receive them within 7 days from the date you sign the form. You may not get expedited Food Supplement benefits, if eligible, until we get a completed application form and interview you.
YOUR SIGNATURE
DATE
4. EXPEDITED SERVICES (CUSTOMERS SHOULD NOT WRITE IN THIS AREA – FOR AGENCY USE ONLY)
Applicants who meet the standards below are eligible to receive FSP benefits within 7 days. Customers must be interviewed, either in person or by telephone, in order to determine eligibility for expedited service. The application must be complete, signed, and identity
verified before expedited benefits can be issued. |
|
|
1. Is the total household income this month, before deductions, less than $150 AND household cash/savings $100 or less? □Yes □ No |
||
Estimated |
Household’s monthly rent or mortgage amount |
= $___________ |
|
|
|
Household cash and savings for all members = $__________ |
Appropriate utility standard (SUA, LUA or actual) = $___________ |
|
A. Total income and liquid resources = $__________ |
B. Total shelter costs |
= $___________ |
|
|
|
2. |
Is the total amount for B. (Total shelter costs) greater than the total for A. (Total income and liquid resources)? |
□ Yes |
□ No |
3. |
Are the household members destitute migrant or seasonal farm workers whose cash and savings are $100 or less? |
□Yes |
□ No |
|
If the answer to any of the above questions is yes, this household is potentially eligible for expedited FSP benefits |
||
4. |
If there is another reason why this household should NOT be expedited, list it here: _______________________________________ |
||
|
|
|
|
I certify that I screened this applicant for expedited Food Supplement Program benefits and determined that the household □ was □ was not eligible for expedited issuance at this time.
|
Signature of Case Manager |
|
|
Date |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FOR |
|
|
LDSS Office |
Programs Applied For / Receiving |
|
Assistance Unit |
|
|
|
WORKER |
|
|
|
|
|
|
ID’s |
|
|
|
|
Case Manager’s Name |
|
|
|
|
||
|
USE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
Client ID |
|
|
|
ONLY |
|
|
|
|
|
|
|
|
|
|
|
|
Application/Redetermination Date |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|||
DHR/FIA
5. AUTHORIZED REPRESENTATIVE (IF DESIRED)
First Name |
|
Middle Name |
Last Name |
|
Jr., III, etc. |
|||
|
|
|
|
|
|
|
|
|
Number |
Street |
|
|
City |
|
State |
|
Zip Code |
|
|
|
|
|
|
|
|
+ 4 |
|
|
|
|
|
|
|
||
Telephone Number |
|
Relationship to you |
|
|
||||
|
|
|
|
|
|
|||
Check what you want the representative to do: |
|
|
|
|
||||
|
Complete interview for you |
Cash your check |
Receive your notices |
|
|
|||
|
Sign your application |
Cash your Food benefits |
Receive your Medical Assistance Card |
|||||
6. INDIVIDUAL INFORMATION Complete the section below.
Last Name |
First Name |
|
Middle Name |
|
Jr.,III etc. |
||
|
|
|
|
|
|
|
|
Maiden/Other Name |
Social Security Number |
List Additional Social Security Number |
|
Date of Birth |
|||
|
|
|
|
|
|
||
Sex |
|
Ethnicity* (see below) |
Race* (see below) |
Marital Status |
|||
Male |
Female |
|
|
|
|
|
|
Resident of Maryland |
Due date if pregnant |
Number of babies |
Receiving Prenatal Care? |
||||
YES |
NO |
|
expected? |
YES |
NO |
||
Receiving benefits in another state: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Public Assistance? |
YES |
NO |
Food benefits? |
YES |
NO |
Medical Assistance? |
YES |
NO |
|||||||||||||
U.S. Citizen? |
Student? |
On Strike? |
|
Disabled or |
|
Medical |
|
Medicare |
|
Medicare# |
|||||||||||
YES NO |
YES |
NO |
YES |
NO |
|
Incapacitated? |
|
Insurance? |
|
Part A |
|
|
|||||||||
|
|
|
|
|
|
|
|
YES |
NO |
|
YES NO |
|
|
YES |
NO |
|
|||||
7. MIGRANT WORKER |
|
|
|
|
|
|
8. BOARDER If you are a boarder, fill in this sections: |
||||||||||||||
Are you a migrant worker? |
|
|
|
|
|
|
Number of Meals per Day |
Cost of Meals per Month |
|||||||||||||
|
|
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
8 IMMIGRATION STATUS — If you are not a United States citizen, fill in this section |
|
|
|
|
|||||||||||||||||
INS Status |
|
|
|
Newly Legalized Status Date |
|
Sponsored Alien |
|
|
|
Country of Origin |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
YES NO |
|
|
|
|
|
|
|
||
US Entry Date |
|
|
|
INS Number |
|
|
Maryland uses the Systematic Alien Verification and Eligibility or SAVE |
||||||||||||||
|
|
|
|
|
|
|
|
system through the United States Citizenship and Immigration Service |
|||||||||||||
|
|
|
|
|
|
|
|
(USCIS) formerly known as Immigration and Naturalization Service (INS) |
|||||||||||||
|
|
|
|
|
|
|
|
to verify the alien status of all applicant and recipient |
|||||||||||||
|
|
|
|
|
|
|
|
households. Information received from USCIS may affect your |
|||||||||||||
|
|
|
|
|
|
|
|
household’s eligibility and benefit amount. |
|
|
|||||||||||
9. SCHOOL — If you are in school, fill in this section: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Student Status |
|
|
Educational Level |
|
|
|
|
|
|
|
|
|
Highest Grade Completed |
||||||||
|
|
Elementary |
College |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Secondary |
Other, List:_______________ |
|
|
|
|
|
|
|
|
||||||||||
|
|
|
Expected Graduation Date (If in high |
||||||||||||||||||
Less than |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
school) |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
School Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
School Number |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
School Address |
|
|
|
|
|
City |
|
|
|
|
|
|
|
State |
|
|
Zip Code + 4 |
||||
|
|
|
|
|
|
|
|
||||||||||||||
10. DISABILITY — If you are disabled or incapacitated, what is the disability? |
|
|
|
|
|
|
|
||||||||||||||
*Use the codes below to complete the Race and Ethnicity blocks. Enter each code that applies, using at least one code for each person. Ethnicity Codes: 1= Hispanic or Latino, 2=Not Hispanic/Latino. Race Codes: You can choose one or more race code - 1=American Indian/Alaskan Native, 2=Asian, 3=Black/African American, 4=Native Hawaiian/Pacific Islander, 5=White
Note: You do not have to give information about your race or ethnicity. If you do, it will help show how we obey the Federal Civil Rights Law. We will not use this information to decide if you are eligible. If you do not give us your race, it will not affect your application. The case manager will enter a race code for statistical purposes only. Title VI of the Civil Rights Act of 1964 allows us to ask for this information.
2
DHR/FIA
11. MEDICAL INSURANCE — If you have medical insurance, fill in this section:
Policy Number |
Group Number |
Policy Holder Name |
|
|
|
Relationship to Policy Holder
POLICY HOLDER ADDRESS
Number Street
City
State
Zip Code + 4
Telephone Number
INSURANCE COMPANY
Insurance Company Name
Number Street
City
Union Name
State |
Zip Code + 4 |
Telephone Number |
|
|
|
UNION
Union Local Number
Number Street
City
State
Zip Code + 4
Telephone Number
12.VETERAN INFORMATION — If you are a veteran or a disabled widow or widower, or a disabled child of a deceased veteran, fill in this section:
Veteran’s Name |
Relationship to Veteran |
Veteran’s Status |
Military Service Number |
|
|
|
|
13. MEDICAL EXPENSE
If you are 60 or older, blind or disabled and applying for or receiving Food Supplement Program benefits, do you have
medical bills that you must pay? |
YES |
NO |
If Yes, bring in your bills. |
|
|
|
||
14. LIQUID ASSETS — Complete for assets as of the 1st day of the month. Check Yes or No for each ASSET TYPE |
||||||||
|
|
|
|
|
AMOUNT |
ACCOUNT |
FDIC |
INSTITUTION |
ASSET TYPE |
|
CHECK ONE |
OWNER |
Balance/value |
NUMBER |
NUMBER |
|
|
Cash on Hand |
|
YES |
NO |
|
$ |
N/A |
N/A |
N/A |
|
|
|
|
|
|
|
|
|
Checking Accounts |
|
YES |
NO |
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
Savings Accounts |
|
YES |
NO |
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
Credit Union Accounts |
|
YES |
NO |
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
Trust Funds |
|
YES |
NO |
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
IRA or Keogh Accounts |
|
YES |
NO |
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
Stocks, bonds, Certificates, |
|
YES |
NO |
|
$ |
|
|
|
Money Market Funds, |
|
|
|
|
|
|
|
|
mutual funds, treasury or |
|
|
|
|
|
|
|
|
Other Notes |
|
|
|
|
|
|
|
|
Annuities: |
|
YES |
NO |
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
Other, List: |
|
YES |
NO |
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
Other, List |
|
YES |
NO |
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
Other, List |
|
YES |
NO |
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
3
DHR/FIA
15.LIFE INSURANCE AND FUNERAL PLANS — If you have any life insurance or
NAME OF PERSON |
ORIGINAL FACE |
CURRENT |
POLICY NUMBER |
LIFE |
COMPANY, |
WHO PAYS |
VALUE OR |
CASH |
OR ACCOUNT |
INSURANCE |
FUNERAL HOME |
|
VALUE OF PLAN |
VALUE |
NUMBER |
OR BURIAL |
OR BANK NAME |
|
|
|
|
PLAN |
|
$
$
$
$
16. REAL PROPERTY — If you own property other than where you live, fill in this section. Include burial plots.
Number |
Street |
City |
State |
|
|
Zip Code + 4 |
|
|
|
|
|
|
|
How Used? |
|
Current Fair Market |
Amount Owed Now |
|
Trying to Sell |
|
|
|
|
|
|
YES |
NO |
Number |
Street |
City |
State |
|
|
Zip Code + 4 |
|
|
|
|
|
|
|
How Used? |
|
Current Fair Market |
Amount Owed Now |
|
Trying to Sell |
|
|
|
|
|
|
YES |
NO |
|
|
|
|
|
|
|
17.OTHER ASSETS — If you own other assets not listed, such as antiques, boat, recreational vehicle, coin collections, furs, jewelry, livestock, or stamp collections, fill in this sections:
ASSET TYPE |
|
CURRENT FAIR MARKET VALUE |
AMOUNT OWED |
|
$ |
|
$ |
|
$ |
|
$ |
18.POTENTIAL ASSET OR INCOME — If you are expecting to receive an accident settlement, trust fund, inheritance or other money or property, fill in this section.
Type
Explanation
19.TRANSFER OF ASSETS — if you sold, traded or gave any property, motor vehicles, stocks, bonds, cash or other assets in the past 3 years (5 years for a trust), fill in this sections:
Transfer Date |
Who Received the Asset? |
|
Type of Assets |
|
|
|
|
|
|
Fair Market Value When Transferred |
Amount Received |
Reason for Transfer |
||
20.INCOME FROM WORKING — If you are working now, fill in this section. If not, list the last job held. Include
NAME OF EMPLOYER
(INCLUDE ADDRESS AND PHONE NUMBER)
Rate of Pay
Number of
Hours
Worked
Amount Per Pay Period
How often Received?
if Job Ended,
Date and amount of Last Pay
4
DHR/FIA