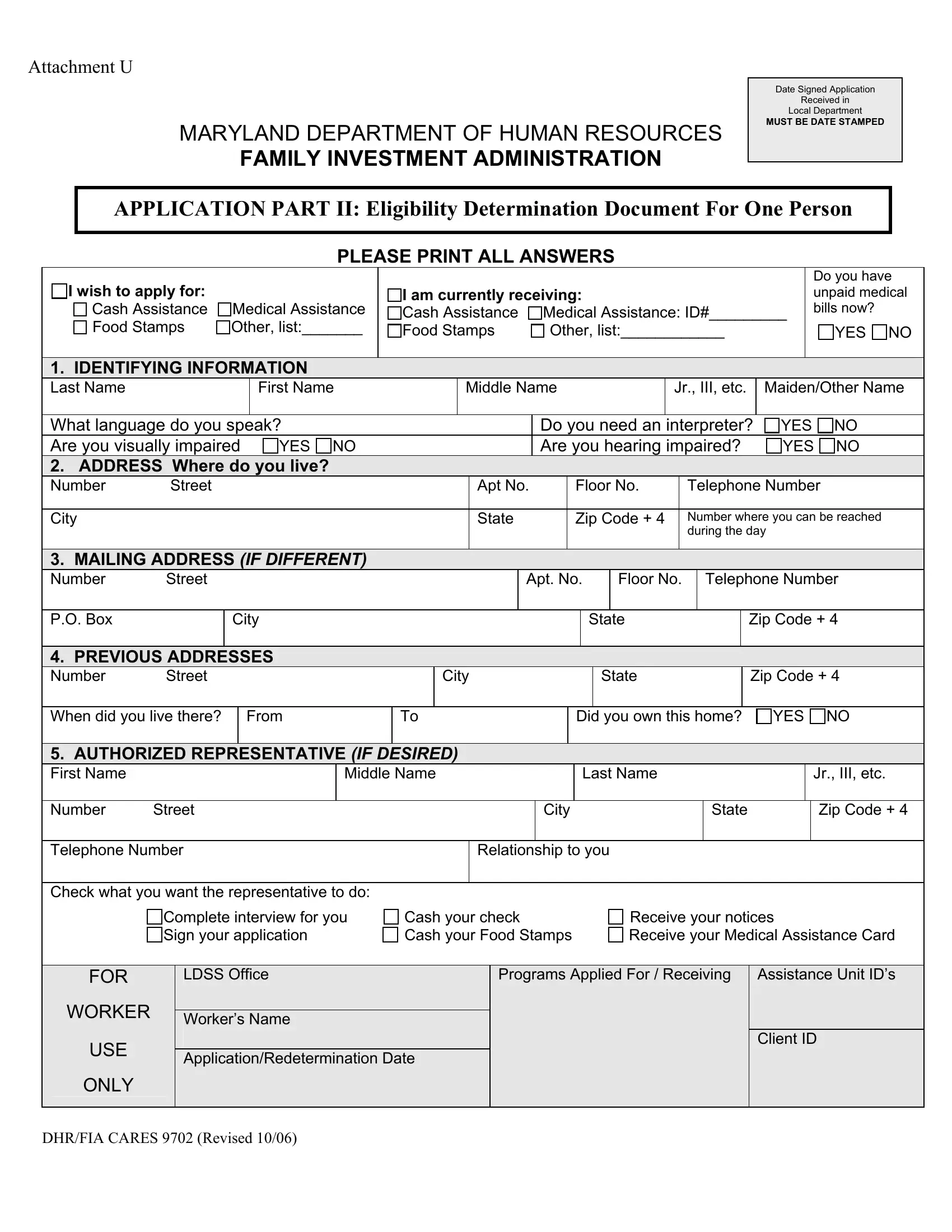
The Dhr Fia Cares 9702 form, a critical document within the Maryland Department of Human Resources Family Investment Administration, serves as a comprehensive tool for eligibility determination for various forms of assistance. Designed meticulously to ensure an intricate yet straightforward application process, the form requires applicants to provide information ranging from personal identification, including names and social security numbers, to in-depth questions about income, assets, disability status, and medical insurance coverage. It also navigates through the applicant's educational background, veteran status, and even details on real property and potential assets or income. The layout of the form intends to capture a holistic view of the applicant's financial and personal situation, addressing essentials like current medical bills, citizenship status, and any representatives that an applicant might have. Additionally, it dives into specifics concerning income from employment, other income sources, benefits, and even the disposition of assets, thereby facilitating a rigorous but fair evaluation of eligibility for assistance programs such as Cash Assistance, Food Stamps, and Medical Assistance. This form is an indispensable part of the application process, underscored by its detailed sections designed to ensure that all necessary information is collected to make an informed and equitable decision regarding assistance eligibility.
| Question | Answer |
|---|---|
| Form Name | Dhr Fia Cares 9702 Form |
| Form Length | 20 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 5 min |
| Other names | HHS, 402-B, MARYLAND, ICD-9-CM |
