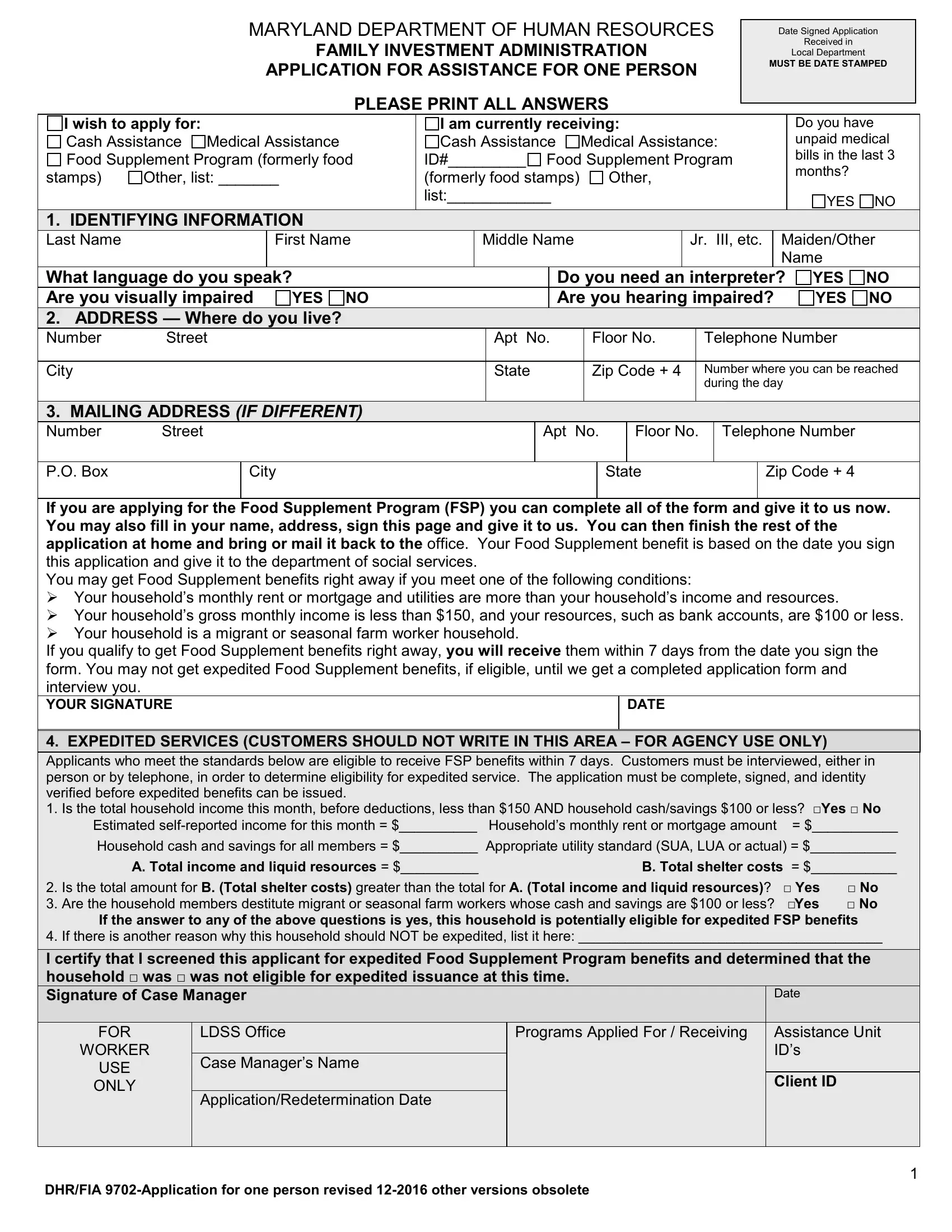
Navigating through the complexities of applying for assistance can often feel overwhelming, but understanding the essentials of forms like the Maryland Department of Human Resources Family Investment Administration Application for Assistance, or as it's formally known, the DHR 9702 form, is a crucial first step. Designed specifically for individuals seeking support, this comprehensive document covers a spectrum of assistance programs including Cash Assistance, Medical Assistance, and the Food Supplement Program, formerly known as food stamps. Required to be date-stamped upon receipt, the form serves as a crucial element in the process, marking the beginning of the applicant's journey towards obtaining necessary aid. Applicants must clearly detail personal information, current assistance received, and whether they have unpaid medical bills, among other specifics. The form also addresses the expedited services for those in immediate need, highlighting the state's commitment to acting swiftly under certain conditions. By demystifying the DHR 9702 form, individuals can more confidently navigate their way through the application process, understanding each section's relevance to their unique circumstances and the broader context of state-supported assistance programs.
| Question | Answer |
|---|---|
| Form Name | Dhr 9702 Form |
| Form Length | 14 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min 30 sec |
| Other names | md dhr application assistance one, dhr fia 9702 one, md dhr fia, dhs fia 9702 |