Our PDF editor that you can take advantage of was designed by our finest web programmers. You may create the ulril file shortly and effortlessly applying our application. Merely keep up with this specific instruction to get going.
Step 1: The first thing is to click the orange "Get Form Now" button.
Step 2: The form editing page is right now available. You can add text or change existing information.
You will have to provide the next data so you can prepare the template:
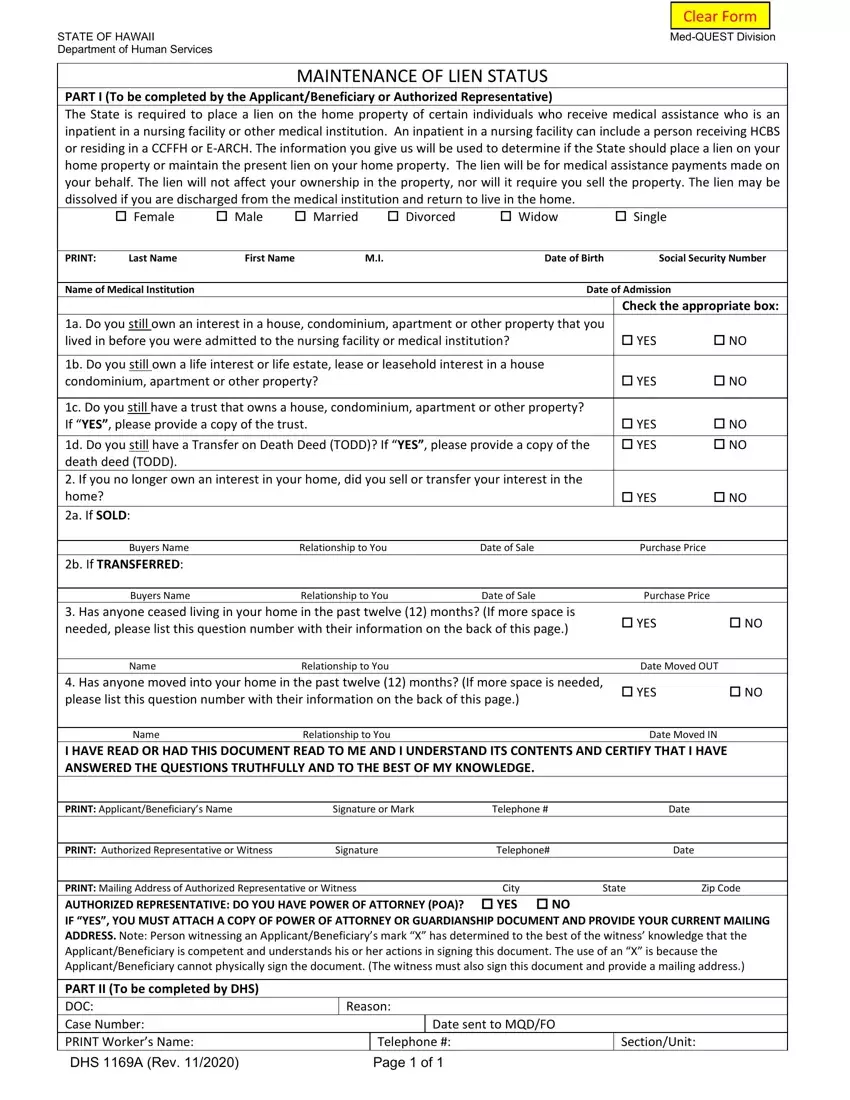
Feel free to fill in the c Do you still have a trust that, YES NO, Buyers Name Relationship to You, Buyers Name Relationship to You, YES NO, Name Relationship to You Date, YES NO, Name Relationship to You Date, PRINT ApplicantBeneficiarys Name, PRINT Authorized Representative or, and PRINT Mailing Address of field with the demanded data.
It is vital to record certain details inside the space PART II To be completed by DHS DOC, Reason, Date sent to MQDFO, Telephone Page of, and SectionUnit.

Step 3: Press the "Done" button. It's now possible to transfer your PDF form to your gadget. As well as that, it is possible to deliver it by means of email.
Step 4: To avoid any specific complications as time goes on, be sure to create a minimum of a couple of duplicates of the form.
