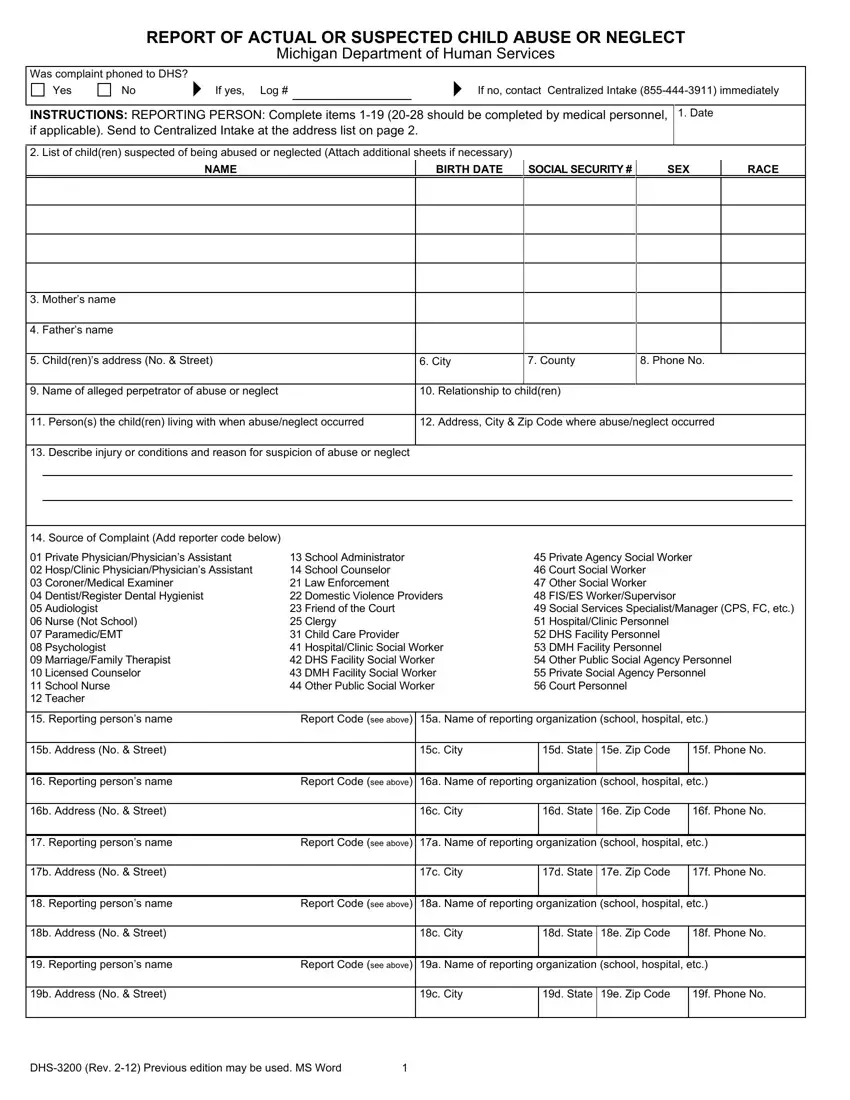
The DHS 3200 form, an integral document issued by the Michigan Department of Human Services, represents a critical mechanism in the fight against child abuse and neglect. This form serves as a structured report for individuals to document and submit instances of actual or suspected child abuse or neglect. Central to safeguarding the welfare of children, the form requires detailed information about the child or children in question, including names, birth dates, and other demographic data, to facilitate a comprehensive understanding and appropriate action by the authorities. Further enriching the form's utility, sections are devoted to the identification of the alleged abuser or neglecter, detailing their relationship to the child, which is pivotal in guiding the subsequent investigation. Importantly, the form acknowledges the crucial role of medical personnel by reserving a segment exclusively for their input, especially when physical examinations reveal abuse or neglect. Designed with inclusivity in mind, it emphasizes non-discrimination and accommodates individuals who require assistance due to disabilities. The robust process outlined for submission, including options for mailing, faxing, and emailing the form, ensures that the mechanism for reporting is accessible and responsive. Highlighting the mandatory nature of this report delineates its significance within the legal framework designed to protect children, making it clear that the state takes these reports seriously, aiming for a thorough assessment and prompt action to safeguard vulnerable members of the community.
| Question | Answer |
|---|---|
| Form Name | DHS-3200 Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 96 |
| Avg. time to fill out | 19 min 46 sec |
| Other names | 3200 form, dhs michigan form 3200, michigan dhs 3200, 3200 form michigan |
