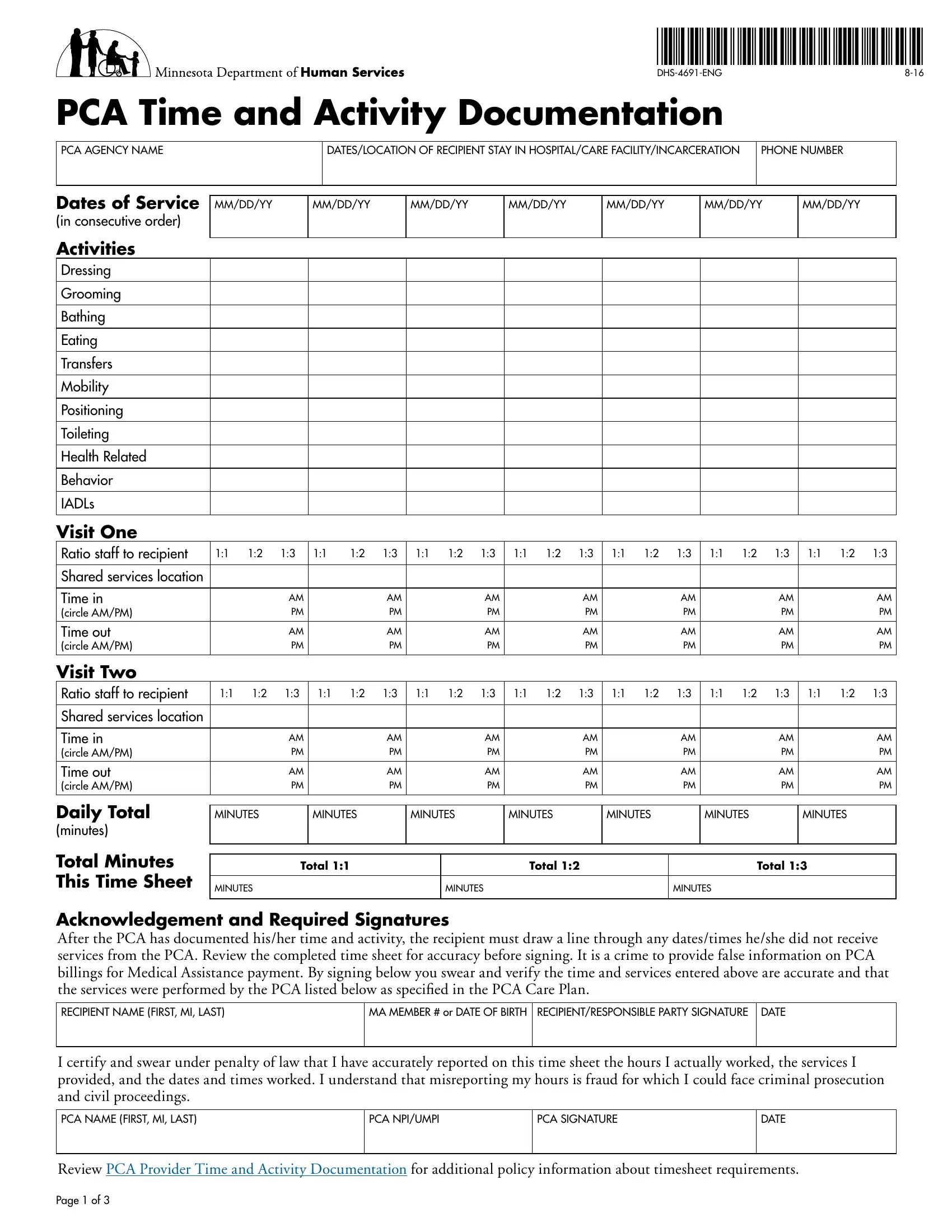
Within the realm of personal care assistance, documentation serves as a cornerstone, ensuring that services provided are thoroughly tracked and accurately billed. The DHS-4691-ENG form is a critical tool in this process, designed to document the time and activities spent by a Personal Care Assistant (PCA) with a recipient. This form records dates of service, types of activities performed, and time spent on each activity, including dressing, grooming, bathing, and more, in a structured manner. It demands meticulous input of dates in consecutive order, with a requirement for activities to be initialed only once per day regardless of the frequency, underscoring the importance of precision in reporting. Furthermore, it accommodates documentation of up to two visits per day, specifying the staff-to-recipient ratio for each visit—an essential metric for shared services. Additionally, it includes sections for recording hospital stays, care facility stays, or periods of incarceration, providing a comprehensive view of the recipient's care continuity. The form culminates with a mandatory acknowledgment and signature section for both the recipient (or responsible party) and the PCA, emphasizing the legal obligation to report accurately and truthfully. This mandatory verification process underpins the form's role in mitigating fraud within the personal care assistance system. Beyond its primary function, the DHS-4691-ENG form also serves as a testament to the commitment to uphold the integrity of personal care services, ensuring recipients receive the care prescribed in their PCA Care Plan.
| Question | Answer |
|---|---|
| Form Name | Dhs 4691 Eng Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | dhs 4691 eng, time activity documentation, pca activity documentation, mn pca time activity |