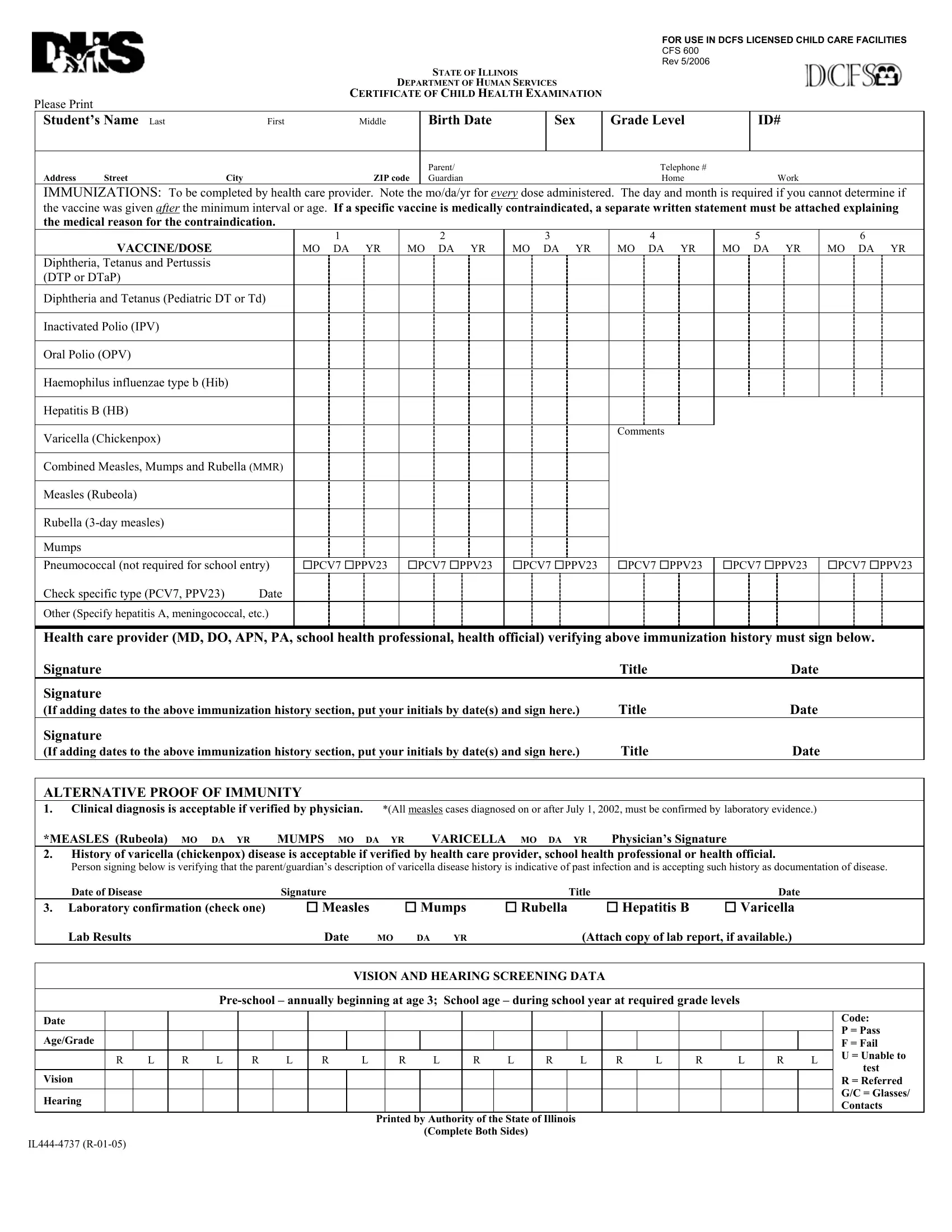
In today's fast-paced world, ensuring the health and safety of children in licensed child care facilities is paramount. The State of Illinois, in cognizance of this fact, mandates the use of the DHS CFS 600 form, a comprehensive Certificate of Child Health Examination that serves as a crucial document in this protective measure. Designed for use in DCFS licensed child care facilities, this form encapsulates detailed health records, including immunizations, vision and hearing screening data, and a thorough health history. It navigates through the labyrinth of health checkpoints starting from immunization records, meticulously documented by healthcare providers, to alternative proofs of immunity against diseases such as measles, mumps, and varicella. Moreover, the form delves into vision and hearing screenings, signifying the importance of these sensory functionalities in a child’s development. The exhaustive health history section, to be filled by parents or guardians and verified by health care providers, highlights allergies, medication, significant medical events or conditions, and family health history. The physical examination section further scrutinizes the child's health status across a spectrum of parameters including lead exposure risk, TB skin test recommendations, and a systemic review, thereby shaping a holistic portrayal of the child’s health landscape. This form acts not just as a procedural necessity but as a beacon of preventive healthcare, aiming to safeguard the well-being of children in day care settings, thereby reassuring parents and guardians of the attentive care their children receive while away from home.
| Question | Answer |
|---|---|
| Form Name | Dhs Form Cfs 600 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Inactivated, cfs600 form, CDC, ILLINOIS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FOR USE IN DCFS LICENSED CHILD CARE FACILITIES |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CFS 600 |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REV 5/2006 |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
STATE OF ILLINOIS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
DEPARTMENT OF HUMAN SERVICES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Please Print |
|
|
|
CERTIFICATE OF CHILD HEALTH EXAMINATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Student’s Name Last |
First |
|
Middle |
|
|
|
Birth Date |
|
Sex |
|
Grade Level |
|
ID# |
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Parent/ |
|
|
|
|
|
|
|
|
Telephone # |
|
|
|
|
|
|
|
|
|||
Address |
Street |
City |
|
|
ZIP code |
|
Guardian |
|
|
|
|
|
|
Home |
|
|
|
Work |
|
|
|
||||||||
IMMUNIZATIONS: To be completed by health care provider. Note the mo/da/yr for every dose administered. The day and month is required if you cannot determine if |
|||||||||||||||||||||||||||||
the vaccine was given after the minimum interval or age. If a specific vaccine is medically contraindicated, a separate written statement must be attached explaining |
|||||||||||||||||||||||||||||
the medical reason for the contraindication. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
1 |
|
|
|
|
|
2 |
|
|
3 |
|
|
|
4 |
|
|
5 |
|
|
|
6 |
|
|
||||
|
VACCINE/DOSE |
|
MO DA |
|
YR |
|
MO |
|
DA |
|
YR |
MO DA |
|
YR |
|
MO DA |
|
YR |
MO DA |
|
|
YR |
MO DA |
|
YR |
||||
Diphtheria, Tetanus and Pertussis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(DTP or DTaP) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diphtheria and Tetanus (Pediatric DT or Td) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inactivated Polio (IPV) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Oral Polio (OPV) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Haemophilus influenzae type b (Hib) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hepatitis B (HB) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Varicella (Chickenpox) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Comments |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Combined Measles, Mumps and Rubella (MMR) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Measles (Rubeola) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rubella |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mumps |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Pneumococcal (not required for school entry) |
PCV7 |
PPV23 |
|
PCV7 |
PPV23 |
PCV7 |
PPV23 |
|
PCV7 |
PPV23 |
PCV7 |
PPV23 |
PCV7 |
PPV23 |
|||||||||||||||
Check specific type (PCV7, PPV23) |
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other (Specify hepatitis A, meningococcal, etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Health care provider (MD, DO, APN, PA, school health professional, health official) verifying above immunization history must sign below.
|
Signature |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Title |
|
|
|
|
|
|
|
Date |
|
||||
|
Signature |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
(If adding dates to the above immunization history section, put your initials by date(s) and sign here.) |
Title |
|
|
|
|
|
|
|
Date |
|
||||||||||||||||||||||||
|
Signature |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
(If adding dates to the above immunization history section, put your initials by date(s) and sign here.) |
Title |
|
|
|
|
|
|
|
Date |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ALTERNATIVE PROOF OF IMMUNITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
1. Clinical diagnosis is acceptable if verified by physician. |
*(All measles cases diagnosed on or after July 1, 2002, must be confirmed by laboratory evidence.) |
|
||||||||||||||||||||||||||||||||
|
*MEASLES (Rubeola) |
MO |
DA |
YR |
MUMPS |
MO DA YR |
|
VARICELLA |
|
MO DA |
YR |
Physician’s Signature |
|
|
|
|
|
|
|||||||||||||||||
|
2. History of varicella (chickenpox) disease is acceptable if verified by health care provider, school health professional or health official. |
|
|
|
|
||||||||||||||||||||||||||||||
|
Person signing below is verifying that the parent/guardian’s description of varicella disease history is indicative of past infection and is accepting such history as documentation of disease. |
||||||||||||||||||||||||||||||||||
|
Date of Disease |
|
|
|
|
Signature |
|
|
|
|
|
|
|
|
|
|
|
|
Title |
|
|
|
|
|
|
|
|
Date |
|
||||||
|
3. Laboratory confirmation (check one) |
|
Measles |
|
|
|
Mumps |
|
Rubella |
|
|
Hepatitis B |
|
|
Varicella |
|
|||||||||||||||||||
|
Lab Results |
|
|
|
|
|
Date |
MO |
DA |
YR |
|
|
|
(Attach copy of lab report, if available.) |
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
VISION AND HEARING SCREENING DATA |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Code: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P = Pass |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Age/Grade |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F = Fail |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
L |
R |
L |
R |
L |
R |
|
L |
|
R |
|
L |
|
R |
L |
|
R |
L |
|
R |
L |
|
R |
L |
|
R |
|
L |
U = Unable to |
||||
|
|
|
|
|
|
|
|
|
|
|
test |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vision |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R = Referred |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
G/C = Glasses/ |
|
Hearing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Contacts |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Printed by Authority of the State of Illinois |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Complete Both Sides) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||