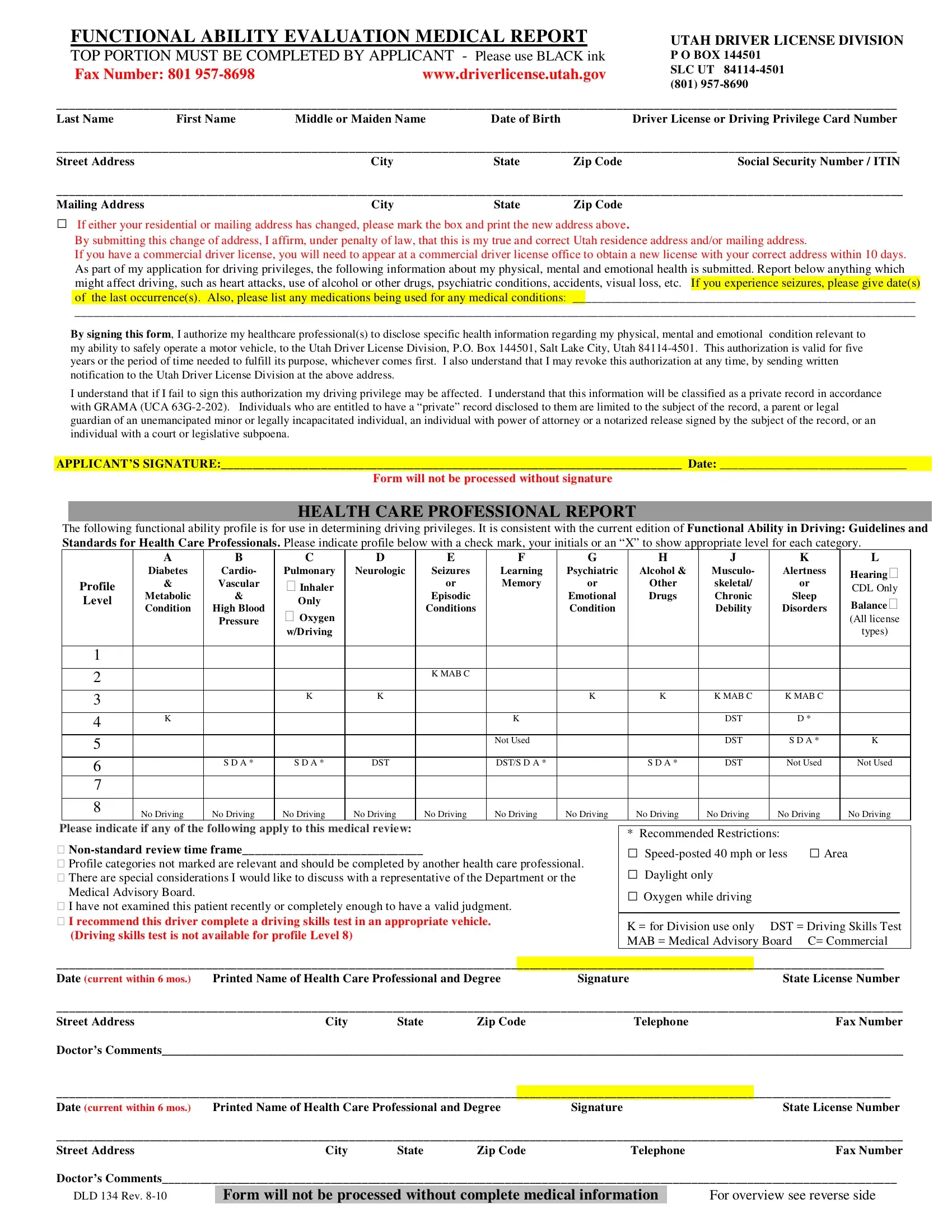
The DLD 134 form, also known as the Functional Ability Evaluation Medical Report, is an essential document for individuals seeking to apply for or renew driving privileges in Utah. It plays a pivotal role in ensuring the safety of both the applicant and the public by assessing the physical, mental, and emotional health of the driver. The form requires the applicant to provide detailed personal information, including their name, address, social security number or ITIN, and any changes to their residential or mailing address. Moreover, applicants must disclose any health conditions or medications that could affect their driving ability, such as heart conditions, use of alcohol or drugs, psychiatric conditions, visual impairments, seizures, and more. This comprehensive evaluation extends to the healthcare professional's perspective, who must fill out a functional ability profile based on current standards and guidelines, indicating any recommended restrictions or necessary tests. The DLD 134 form emphasizes the collaborative effort between the applicant, healthcare professionals, and the Utah Driver License Division to maintain road safety while addressing the individual needs of drivers.
| Question | Answer |
|---|---|
| Form Name | Dld 134 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | dld 134 form, dld 134 rev 5 18, utah, DST |
