
Any time you need to fill out dmas 97ab form plan of care, there's no need to install any programs - simply make use of our PDF tool. We at FormsPal are aimed at giving you the absolute best experience with our tool by continuously presenting new functions and upgrades. Our tool has become a lot more useful with the most recent updates! Currently, filling out PDF documents is easier and faster than ever before. If you are looking to get started, here's what it requires:
Step 1: Firstly, open the pdf tool by clicking the "Get Form Button" at the top of this page.
Step 2: When you launch the PDF editor, you will get the document prepared to be filled out. In addition to filling in different fields, you might also perform other things with the file, such as adding your own words, changing the initial text, inserting images, placing your signature to the form, and much more.
Completing this PDF needs attention to detail. Ensure that each and every blank is done properly.
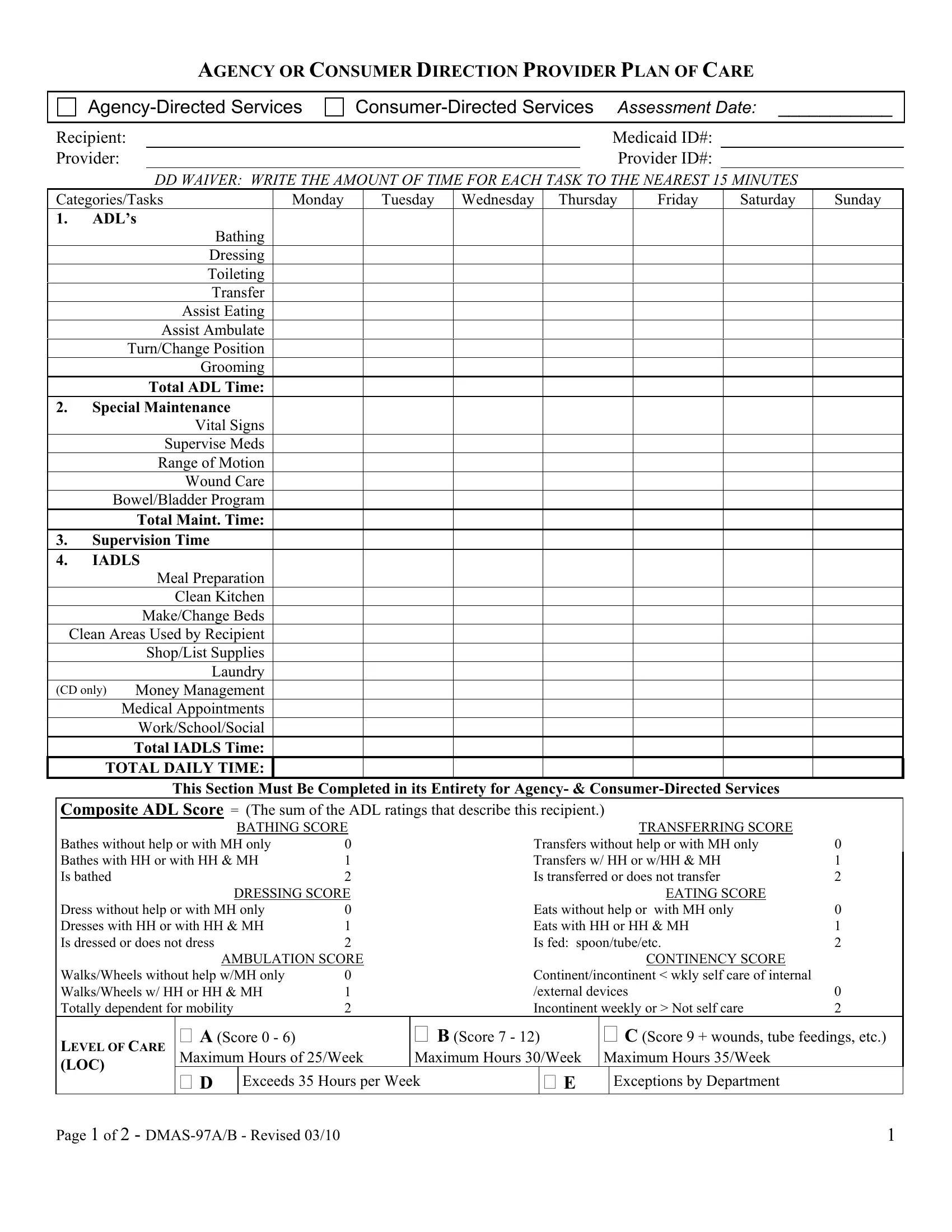
1. To start off, once filling in the dmas 97ab form plan of care, start in the section containing subsequent blank fields:

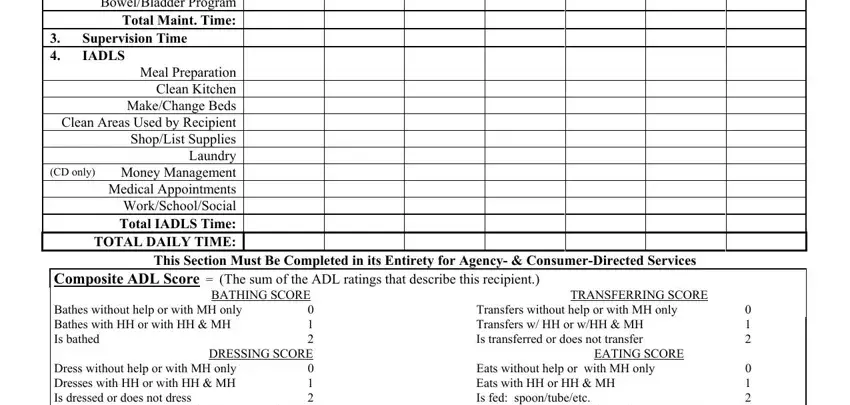
2. Given that the previous array of fields is complete, you're ready to include the necessary specifics in CategoriesTasks ADLs, Vital Signs Supervise Meds Range, Supervision Time IADLS, Meal Preparation Clean Kitchen, This Section Must Be Completed in, Composite ADL Score The sum of, BATHING SCORE, TRANSFERRING SCORE, Bathes without help or with MH, Dress without help or with MH only, DRESSING SCORE, Transfers without help or with MH, EATING SCORE, and Eats without help or with MH only so that you can move forward to the third part.
3. The next part should be pretty uncomplicated, WalksWheels without help wMH only, LEVEL OF CARE LOC, A Score Maximum Hours of Week, Exceeds Hours per Week, Continentincontinent wkly self, B Score, C Score wounds tube feedings etc, Maximum Hours Week Maximum Hours, Page of DMASAB Revised, and Exceptions by Department - all these empty fields is required to be completed here.
4. The following paragraph needs your information in the subsequent parts: Recipient Provider, Medicaid ID Provider ID, Initial Plan of Care hours must be, Reason Plan of Care Submitted New, In Hours In Hours, Transfer, Documentation must support the, Reason for changeadditional, Backup Plan Persons name for CD, Plan of Care Effective Date, Recipient Care Giver Signature, RN or SF Signature, Total Weekly Hours, Date, and Date. Make certain to enter all of the requested information to move further.
5. This form must be finished within this segment. Further there can be found a detailed listing of blank fields that need accurate details to allow your document usage to be faultless: Provider Notification To Client, Instructions for Completion of the, CategoryTasks, FOR DD WAIVER ONLY Write the, Level of Care Determination For, Enter a score for each activity of, Provider Notification To Client, Anytime the RN Supervisor or, PA Contractor Notification To, If the changes to the Plan of Care, Recipient Care Giver Signature, and The recipients signature is.
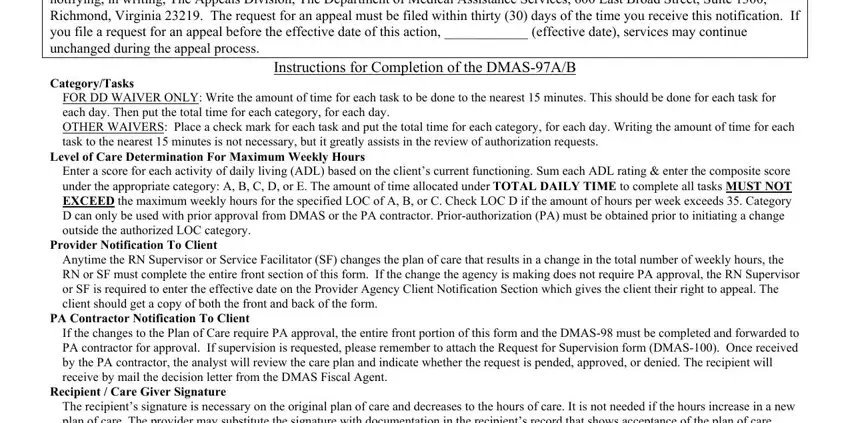
Always be really attentive while filling in Instructions for Completion of the and If the changes to the Plan of Care, because this is the part where most people make errors.
Step 3: Check what you've typed into the blanks and click the "Done" button. After creating afree trial account at FormsPal, you will be able to download dmas 97ab form plan of care or email it without delay. The PDF file will also be accessible in your personal cabinet with all your edits. We do not share any details you type in when completing forms at our site.