
You can fill in durable medical equipment necessity easily using our PDFinity® online PDF tool. In order to make our tool better and more convenient to work with, we constantly design new features, taking into account suggestions from our users. All it requires is just a few simple steps:
Step 1: First of all, access the pdf editor by clicking the "Get Form Button" at the top of this page.
Step 2: The tool lets you modify PDF documents in a variety of ways. Modify it with any text, correct what is originally in the document, and add a signature - all at your disposal!
Pay close attention when completing this document. Make sure all necessary areas are filled in correctly.
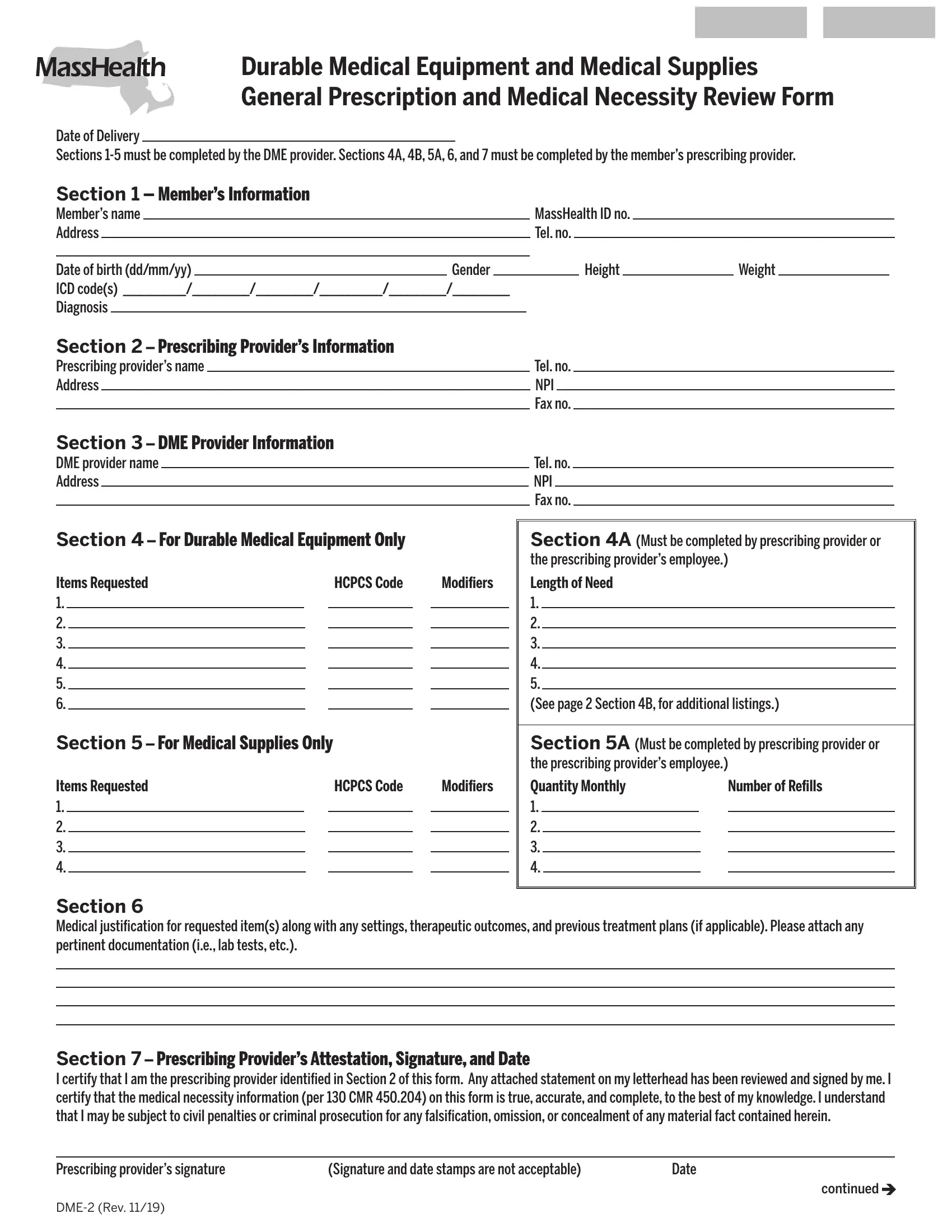
1. You need to complete the durable medical equipment necessity correctly, so take care while filling out the areas comprising these fields:
2. The next part is usually to submit the next few blank fields: Modifiers, Length of Need See page, Section A Must be completed by, Quantity Monthly, Number of Refills, Items Requested, Section For Medical Supplies Only, Items Requested, HCPCS Code, Section Medical justification for, and Section Prescribing Providers.
3. The following portion focuses on ITEMS REQUESTED, Quantity, HCPCS, and Modifier - complete each one of these empty form fields.
4. Now start working on this next segment! Here you've got these Provider of DME Attestation, I certify under the pains and, Provider of DMEs signature, and Printed legal name of provider blanks to complete.
5. When you near the completion of this file, you'll notice several extra requirements that must be satisfied. In particular, Printed legal name of provider, Printed legal name of individual, Date, and page should all be filled out.

People often make errors while completing page in this area. You should reread everything you type in here.
Step 3: Be certain that your information is accurate and press "Done" to continue further. Sign up with FormsPal now and immediately get durable medical equipment necessity, available for downloading. All changes you make are kept , which means you can edit the pdf at a later stage anytime. FormsPal offers safe form tools with no data record-keeping or sharing. Rest assured that your details are safe here!