

Any time you desire to fill out ct p 40, you don't have to install any sort of programs - simply use our online tool. We at FormsPal are devoted to providing you with the best possible experience with our tool by regularly adding new capabilities and enhancements. With these improvements, using our editor gets easier than ever before! In case you are seeking to begin, here is what it will require:
Step 1: Click the orange "Get Form" button above. It'll open our pdf tool so you could start completing your form.
Step 2: Using this online PDF editing tool, you are able to accomplish more than simply fill out blanks. Express yourself and make your docs appear great with custom text added in, or tweak the file's original input to perfection - all that comes with an ability to add any kind of images and sign it off.
With regards to the blank fields of this precise form, here is what you should consider:
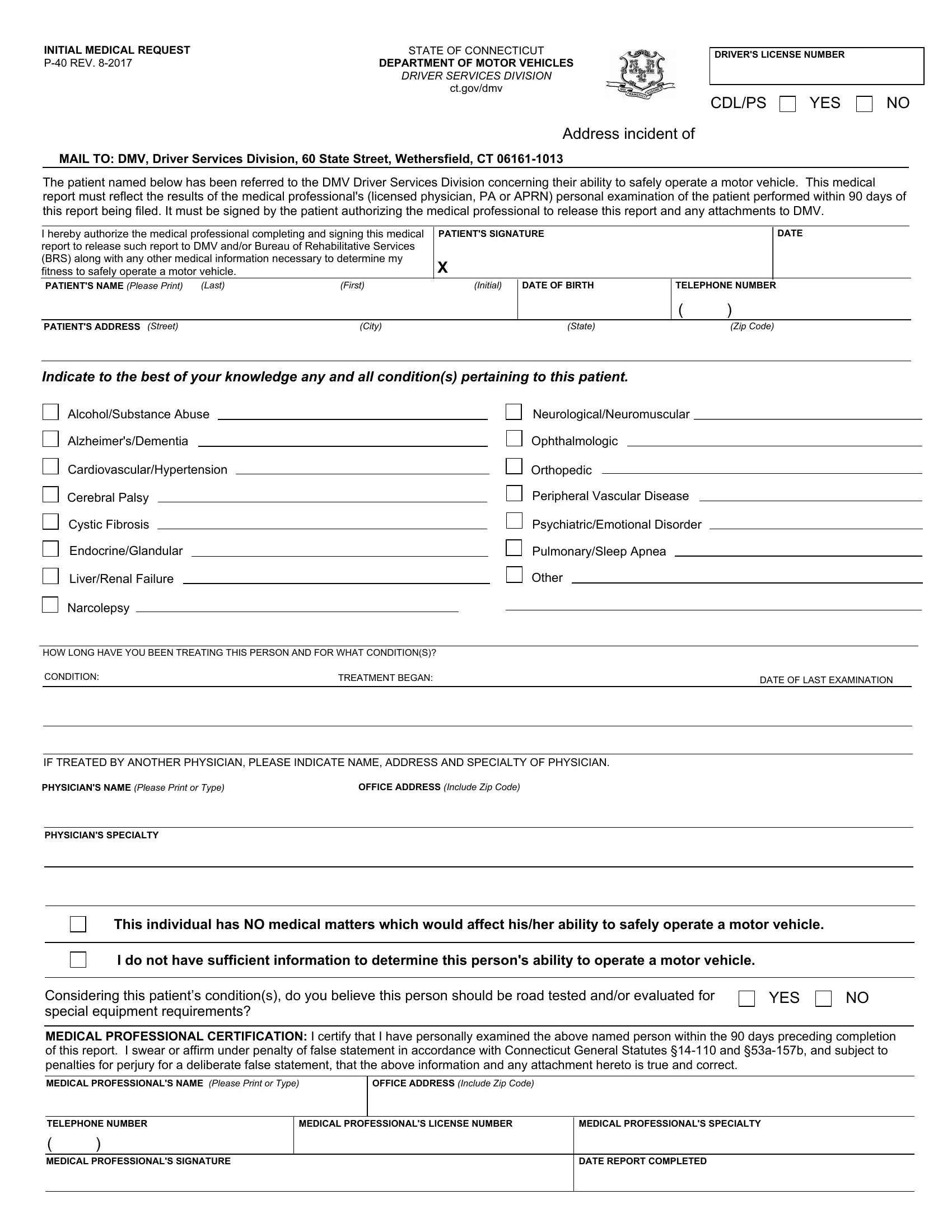
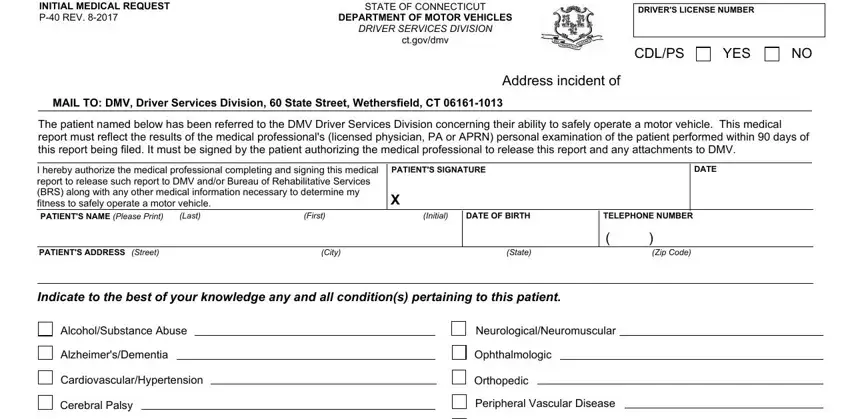
1. Firstly, once filling out the ct p 40, start out with the section containing subsequent fields:
2. Your next step is usually to fill out these particular fields: Cystic Fibrosis, EndocrineGlandular, LiverRenal Failure, Narcolepsy, PsychiatricEmotional Disorder, PulmonarySleep Apnea, Other, HOW LONG HAVE YOU BEEN TREATING, CONDITION, TREATMENT BEGAN, DATE OF LAST EXAMINATION, IF TREATED BY ANOTHER PHYSICIAN, PHYSICIANS NAME Please Print or, OFFICE ADDRESS Include Zip Code, and PHYSICIANS SPECIALTY.
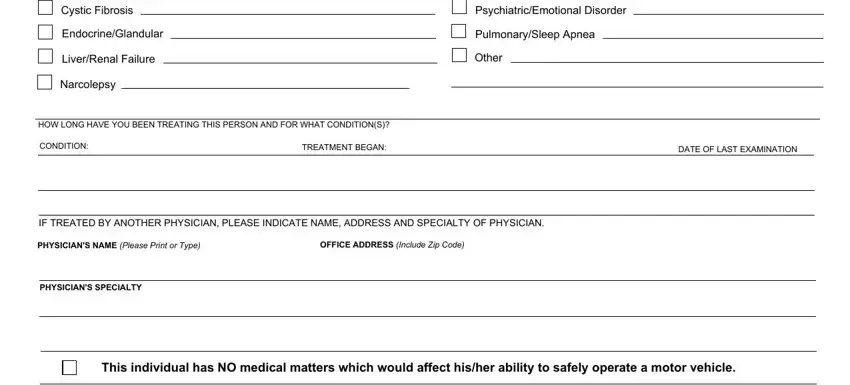
In terms of HOW LONG HAVE YOU BEEN TREATING and IF TREATED BY ANOTHER PHYSICIAN, ensure you review things in this section. Both these are surely the most important fields in the document.
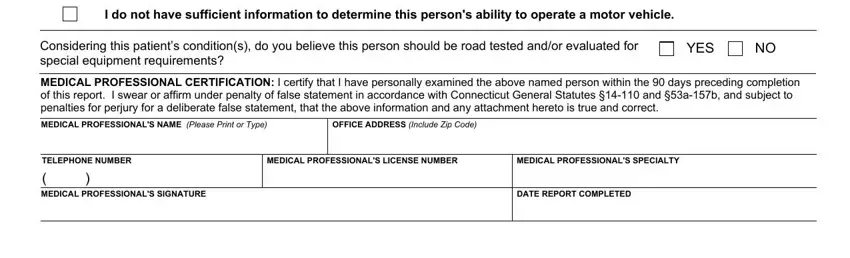
3. In this specific part, take a look at I do not have sufficient, Considering this patients, YES, MEDICAL PROFESSIONAL CERTIFICATION, MEDICAL PROFESSIONALS NAME Please, OFFICE ADDRESS Include Zip Code, TELEPHONE NUMBER, MEDICAL PROFESSIONALS LICENSE, MEDICAL PROFESSIONALS SPECIALTY, MEDICAL PROFESSIONALS SIGNATURE, and DATE REPORT COMPLETED. Each of these have to be filled out with highest accuracy.
Step 3: Prior to finishing the document, make certain that form fields are filled out correctly. As soon as you think it's all fine, click “Done." Right after registering afree trial account with us, you will be able to download ct p 40 or send it via email right off. The PDF will also be readily available in your personal account page with your each and every edit. We do not sell or share any details that you provide when working with documents at FormsPal.