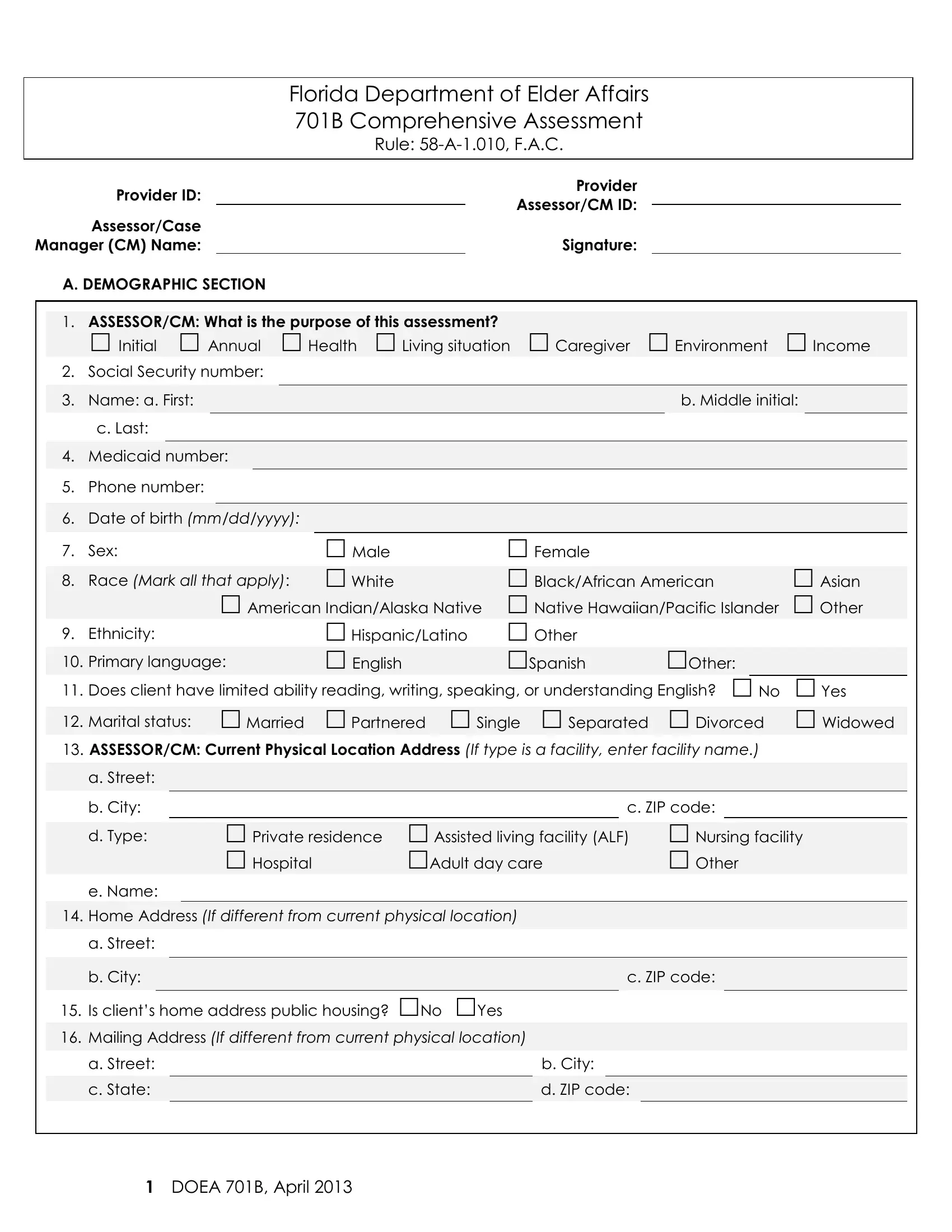
In the realm of elder care and support within the state of Florida, the DOEA 701B Comprehensive Assessment Form emerges as a critical document, articulated by the Florida Department of Elder Affairs. At the heart of this form lies a meticulous gathering of demographic, health, sensory, communication, and daily living activity data, aimed at crafting a nuanced understanding of the elderly's needs. Embarking with sections that traverse through basic identification including social security and Medicaid numbers, it progresses to encapsulate details about the individual's living situation, caregiver dynamics, and their environment. A notable emphasis is placed on assessing the individual's physical health, cognitive capabilities including memory function, as well as sensory and communication abilities, to illuminate any assistance or devices that may be requisite. Moreover, the form inquires into activities of daily living (ADLs), gauging the level of dependence in tasks such as bathing, dressing, and mobility. This thorough evaluation not only underscores the initial, annual, or transitional situations that necessitate the assessment but also carves pathways for tailored care plans, ensuring the elderly receive apt support and resources indispensable for maintaining their dignity and quality of life.
| Question | Answer |
|---|---|
| Form Name | DOEA 701B Form |
| Form Length | 19 pages |
| Fillable? | Yes |
| Fillable fields | 1316 |
| Avg. time to fill out | 38 min 17 sec |
| Other names | 701b, florida 701b training, 701b certification, 701b assessment |
|
|
Florida Department of Elder Affairs |
|||
|
|
701B Comprehensive Assessment |
|||
|
|
Rule: |
|||
|
|
|
|
|
|
Provider ID: |
|
|
Provider |
||
|
Assessor/CM ID: |
|
|
||
Assessor/Case |
|
|
|
||
|
|
|
|
||
Manager (CM) Name: |
|
|
Signature: |
|
|
A. DEMOGRAPHIC SECTION |
|
|
|
|
|
1.ASSESSOR/CM: What is the purpose of this assessment?
|
|
Initial Annual Health Living situation |
Caregiver Environment |
Income |
|
||||||||||||||||||||||
|
2. |
Social Security number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
Name: a. First: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. Middle initial: |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c. Last: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
Medicaid number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
5. |
Phone number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
6. |
Date of birth (mm/dd/yyyy): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
7. |
Sex: |
|
|
Male |
|
Female |
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
8. |
Race (Mark all that apply): |
|
|
White |
|
Black/African American |
|
Asian |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
American Indian/Alaska Native |
|
Native Hawaiian/Pacific Islander |
|
Other |
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
9. |
Ethnicity: |
|
|
Hispanic/Latino |
|
Other |
|
|
|
|
|
|
|
|
||||||||||||
|
10. |
Primary language: |
|
|
English |
|
Spanish |
|
|
Other: |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
11. |
Does client have limited ability reading, writing, speaking, or understanding English? No |
|
Yes |
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
12. |
Marital status: |
|
|
Married |
|
|
Partnered |
Single |
Separated |
|
Divorced |
|
Widowed |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13.ASSESSOR/CM: Current Physical Location Address (If type is a facility, enter facility name.)
a. Street:
|
|
b. City: |
|
|
|
|
|
|
|
|
|
|
c. ZIP code: |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d. Type: |
|
|
|
Private residence |
|
Assisted living facility (ALF) |
|
Nursing facility |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hospital |
|
Adult day care |
|
Other |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
e. Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
14. |
Home Address (If different from current physical location) |
|
|
|
|
||||||||||||||||
|
|
|
|
|
||||||||||||||||||
|
|
a. Street: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
b. City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
c. ZIP code: |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
15. |
Is client’s home address public housing? No Yes |
|
|
|
|
|||||||||||||||||
|
Mailing Address (If different from current physical location) |
|
|
|
|
|||||||||||||||||
|
16. |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
||||||||||||||||||
|
|
a. Street: |
|
|
|
|
|
|
|
b. City: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
c. State: |
|
|
|
|
|
|
|
|
d. ZIP code: |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1DOEA 701B, April 2013