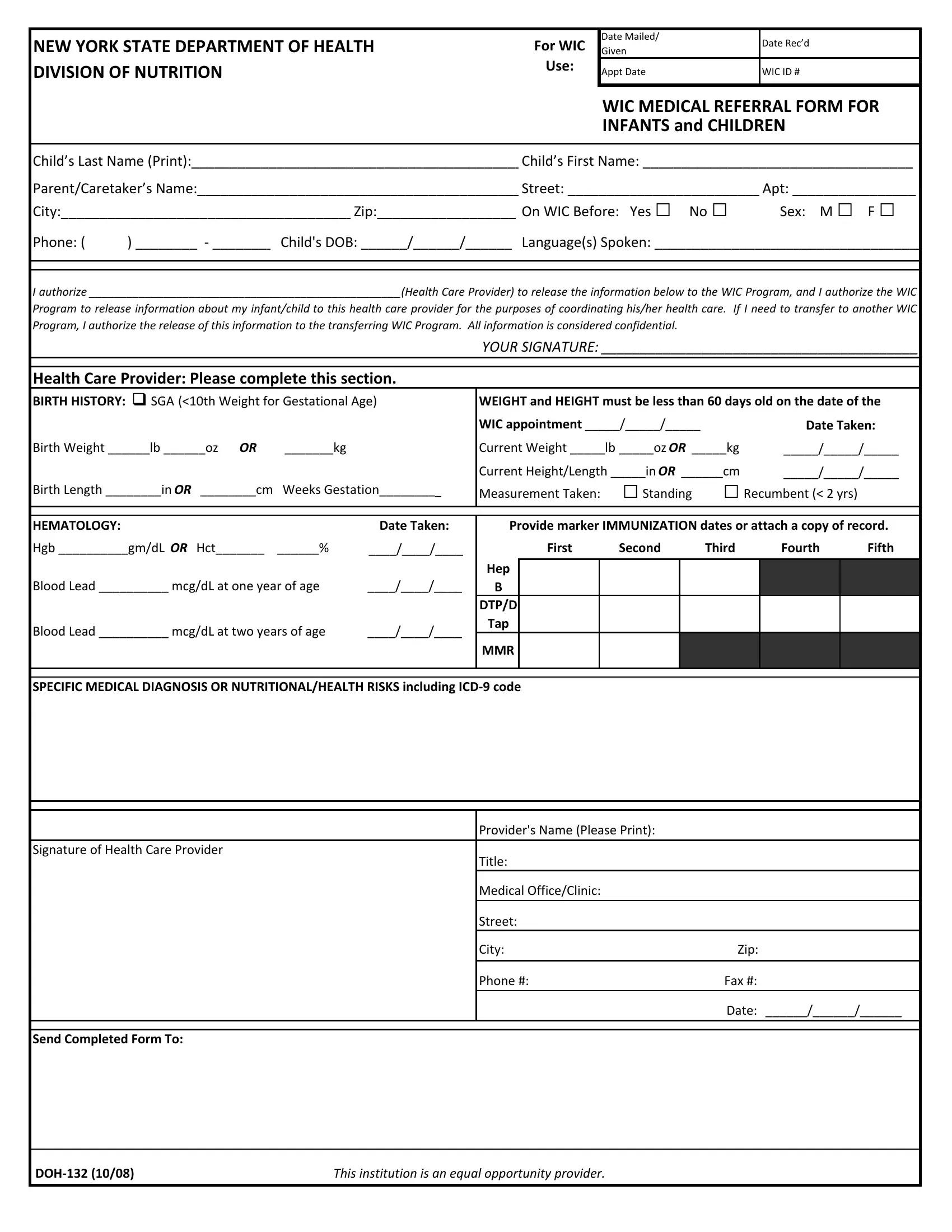
The Department of Health's DOH 132 form serves as a critical junction in the healthcare and nutritional support framework, especially catering to infants and children within New York State’s WIC Program. This comprehensive form not only facilitates a seamless exchange of vital health information between healthcare providers and the WIC (Women, Infants, and Children) Program but also ensures the continuity of care when families transition between WIC programs. The necessity of this form arises from its detailed sections that capture essential data such as the child's birth history, current weight and height, hematology details, and immunization records. This rich dataset empowers WIC nutritionists and counselors to tailor their assistance and advice to meet the specific nutritional needs of each child. Moreover, the inclusion of specific medical diagnosis or nutritional/health risks, along with ICD-9 codes, further refines the scope of care provided. The form underscores the importance of guardian authorization for the release and exchange of medical information, highlighting the program's commitment to confidentiality and privacy. Through its structured format, the DOH 132 form exemplifies a well-thought-out tool for fostering collaborative health care, ensuring that young beneficiaries of the WIC Program receive the most appropriate nutritional support and medical care tailored to their individual needs.
| Question | Answer |
|---|---|
| Form Name | Doh 132 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | wic nyc pdf, Recumbent, MMR, Hct |
NEW YORK STATE DEPARTMENT OF HEALTH |
For WIC |
Date Mailed/ |
Date Rec’d |
|
Given |
||||
|
||||
DIVISION OF NUTRITION |
Use: |
Appt Date |
WIC ID # |
|
|
||||
|
|
|
|
WIC MEDICAL REFERRAL FORM FOR
INFANTS and CHILDREN
Child’s Last Name (Print):___________________________________________ Child’s First Name: ___________________________________
Parent/Caretaker’s Name:__________________________________________ Street: _________________________ Apt: ________________ |
||||
City:______________________________________ Zip:__________________ On WIC Before: Yes □ |
No □ |
Sex: M □ |
F □ |
|
Phone: ( |
) ________ ‐ ________ Child's DOB: ______/______/______ Language(s) Spoken: ___________________________________ |
|||
I authorize __________________________________________________(Health Care Provider) to release the information below to the WIC Program, and I authorize the WIC
Program to release information about my infant/child to this health care provider for the purposes of coordinating his/her health care. If I need to transfer to another WIC Program, I authorize the release of this information to the transferring WIC Program. All information is considered confidential.
YOUR SIGNATURE: _________________________________________
Health Care Provider: Please complete this section.
BIRTH HISTORY: |
SGA (<10th Weight for Gestational Age) |
WEIGHT and HEIGHT must be less than 60 days old on the date of the |
||||||||||
|
|
|
|
WIC appointment _____/_____/_____ |
|
Date Taken: |
||||||
Birth Weight ______lb ______oz OR |
_______kg |
Current Weight _____lb _____oz OR _____kg |
_____/_____/_____ |
|||||||||
|
|
|
|
Current Height/Length _____in OR ______cm |
_____/_____/_____ |
|||||||
Birth Length ________in OR ________cm |
Weeks Gestation_________ |
Measurement Taken: |
□Standing |
□Recumbent (< 2 yrs) |
|
|||||||
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|||
HEMATOLOGY: |
|
|
Date Taken: |
Provide marker IMMUNIZATION dates or attach a copy of record. |
||||||||
Hgb __________gm/dL OR Hct_______ |
______% |
____/____/____ |
|
First |
Second |
Third |
Fourth |
Fifth |
||||
|
|
|
|
Hep |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Blood Lead __________ mcg/dL at one year of age |
____/____/____ |
B |
|
|
|
|
|
|
|
|
||
|
|
|
|
DTP/D |
|
|
|
|
|
|
|
|
Blood Lead __________ mcg/dL at two years of age |
____/____/____ |
Tap |
|
|
|
|
|
|
|
|
||
MMR |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
||||||
SPECIFIC MEDICAL DIAGNOSIS OR NUTRITIONAL/HEALTH RISKS including ICD‐9 code |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Provider's Name (Please Print): |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of Health Care Provider |
|
|
Title: |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
Medical Office/Clinic: |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Street: |
|
|
|
|
|
|
||
|
|
|
|
City: |
|
|
Zip: |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Phone #: |
|
|
Fax #: |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
Date: ______/______/______ |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Send Completed Form To: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
DOH‐132 (10/08) |
|
|
This institution is an equal opportunity provider. |
|
|
|
|
|
|
|||