
doh release of information form can be completed online effortlessly. Just try FormsPal PDF editor to complete the task without delay. The editor is continually maintained by us, getting powerful features and becoming better. Getting underway is simple! All you should do is stick to these simple steps directly below:
Step 1: Open the PDF form in our editor by pressing the "Get Form Button" at the top of this page.
Step 2: The tool allows you to modify most PDF forms in various ways. Improve it by writing customized text, adjust what is already in the PDF, and include a signature - all manageable within a few minutes!
Completing this PDF will require attention to detail. Make certain all mandatory blank fields are filled out properly.
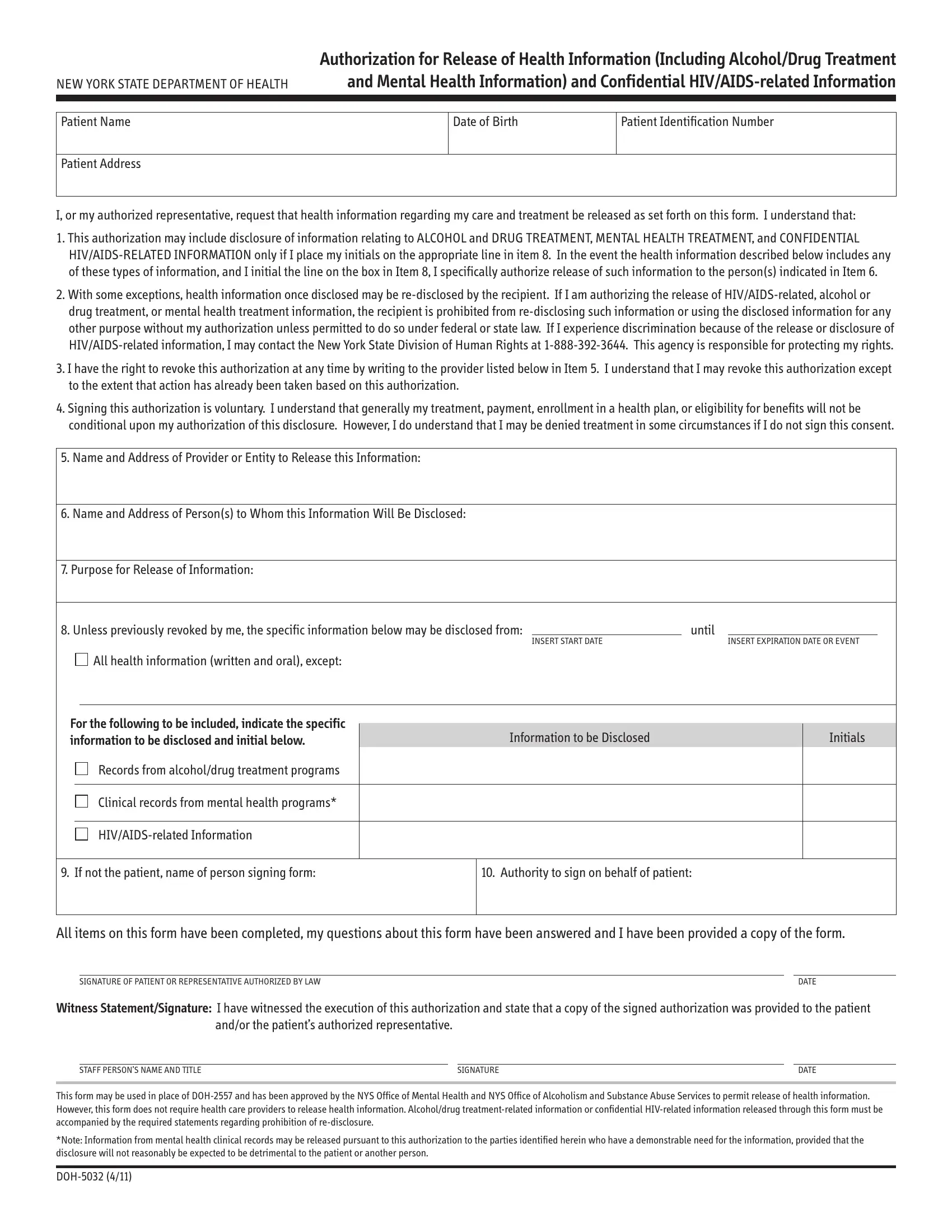
1. The doh release of information form requires certain details to be inserted. Ensure the next fields are finalized:
2. Once your current task is complete, take the next step – fill out all of these fields - Unless previously revoked by me, INSERT START DATE, until, INSERT EXPIRATION DATE OR EVENT, All health information written and, For the following to be included, Records from alcoholdrug treatment, Clinical records from mental, HIVAIDSrelated Information, Information to be Disclosed, Initials, If not the patient name of, Authority to sign on behalf of, All items on this form have been, and SIGNATURE OF PATIENT OR with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
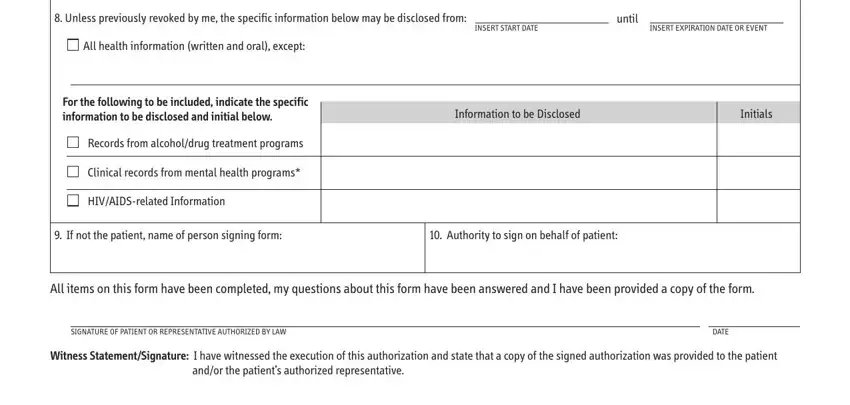
Be very careful when filling out Information to be Disclosed and until, as this is the section in which many people make mistakes.
Step 3: You should make sure your details are correct and then click "Done" to complete the task. Get hold of the doh release of information form after you sign up for a free trial. Instantly use the document in your FormsPal cabinet, together with any modifications and adjustments automatically kept! FormsPal guarantees your information privacy with a secure system that never saves or shares any personal information involved in the process. Rest assured knowing your paperwork are kept protected each time you use our tools!