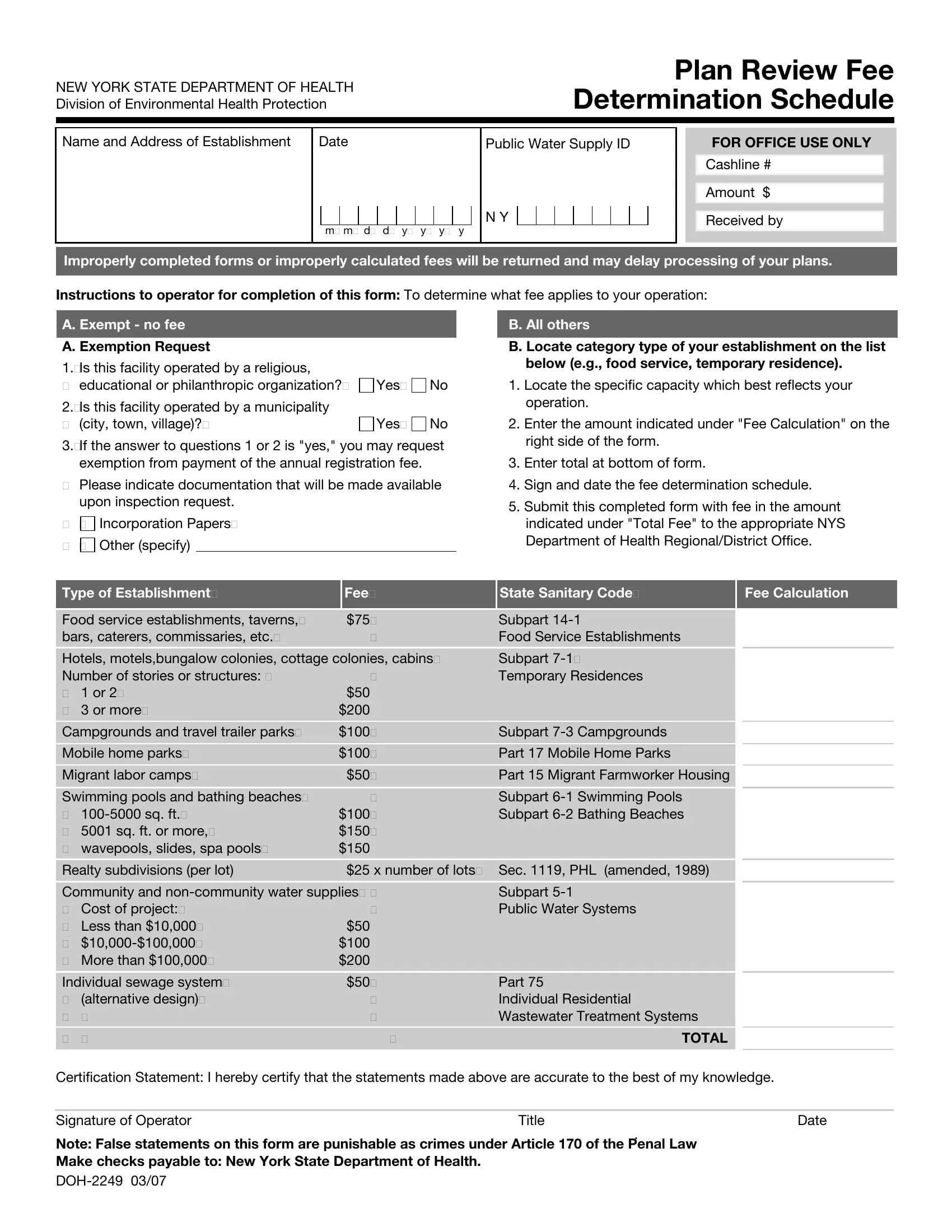
The New York State Department of Health, Division of Environmental Health Protection, has created an essential document known as the DOH 2249 form, which plays a pivotal role for operators and establishments seeking to determine their required fee for plan review. At its core, this form provides a structured method for calculating fees associated with various establishment types, ranging from food service establishments and temporary residences to public water systems and individual sewage systems. Operators are required to specify the nature and capacity of their operation, then calculate the corresponding fee from a defined schedule. Additionally, the form accommodates requests for exemptions, applicable to entities operated by religious, educational, philanthropic organizations, or municipalities, under certain conditions. To streamline the review process, the DOH requires accurate completion and submission of this form, alongside the appropriate fee, to the relevant regional or district health office. Improperly completed forms or inaccurately calculated fees will lead to delays, underscoring the importance of attention to detail in this administrative procedure. Those found making false statements on this form face legal consequences, emphasizing the seriousness with which the Department of Health approaches this aspect of environmental health protection.
| Question | Answer |
|---|---|
| Form Name | Form Doh 2249 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | doh 2249 doh2249 form |
