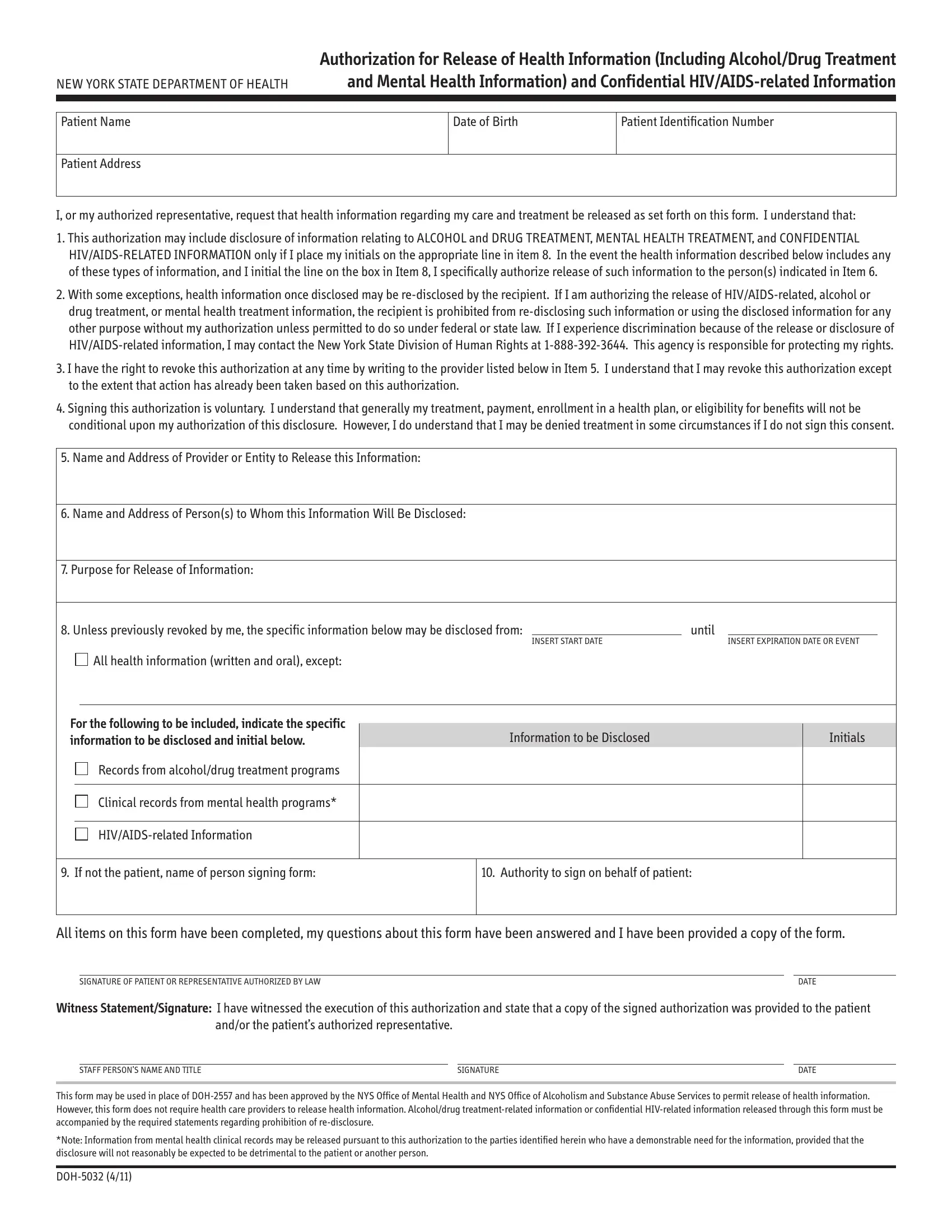
The Doh 5032 form, known as the Authorization for Release of Health Information (Including Alcohol/Drug Treatment and Mental Health Information) and Confidential HIV/AIDS-related Information, plays a critical role in the healthcare sector in New York State. Developed by the New York State Department of Health, this document empowers patients or their authorized representatives to request the release of their health information under specific conditions. It covers a wide range of sensitive information, including details pertaining to alcohol and drug treatment, mental health treatment, and confidential HIV/AIDS-related information, requiring the patient's initials for the release of each type. The form highlights the possibility of the re-disclosure of information by the recipient with certain legal exceptions and stresses the patient's right to non-discrimination and to revoke the authorization at any moment. Explicitly, it emphasizes the voluntary nature of signing this authorization, clarifying that it generally does not affect the patient’s access to treatment, payment, or eligibility for benefits, with specified exceptions. The DOH-5032 form, which supersedes previous forms for similar purposes, mandates the inclusion of detailed information like the identification of the provider, the recipient of the information, the purpose of the release, and the duration for which the release is valid, ensuring a comprehensive and secure process for the sharing of vital health information.
| Question | Answer |
|---|---|
| Form Name | Doh Form 5032 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | doh 5032 form, 5032 form, doh confidential, authorization for release of health info form doh 5032 |