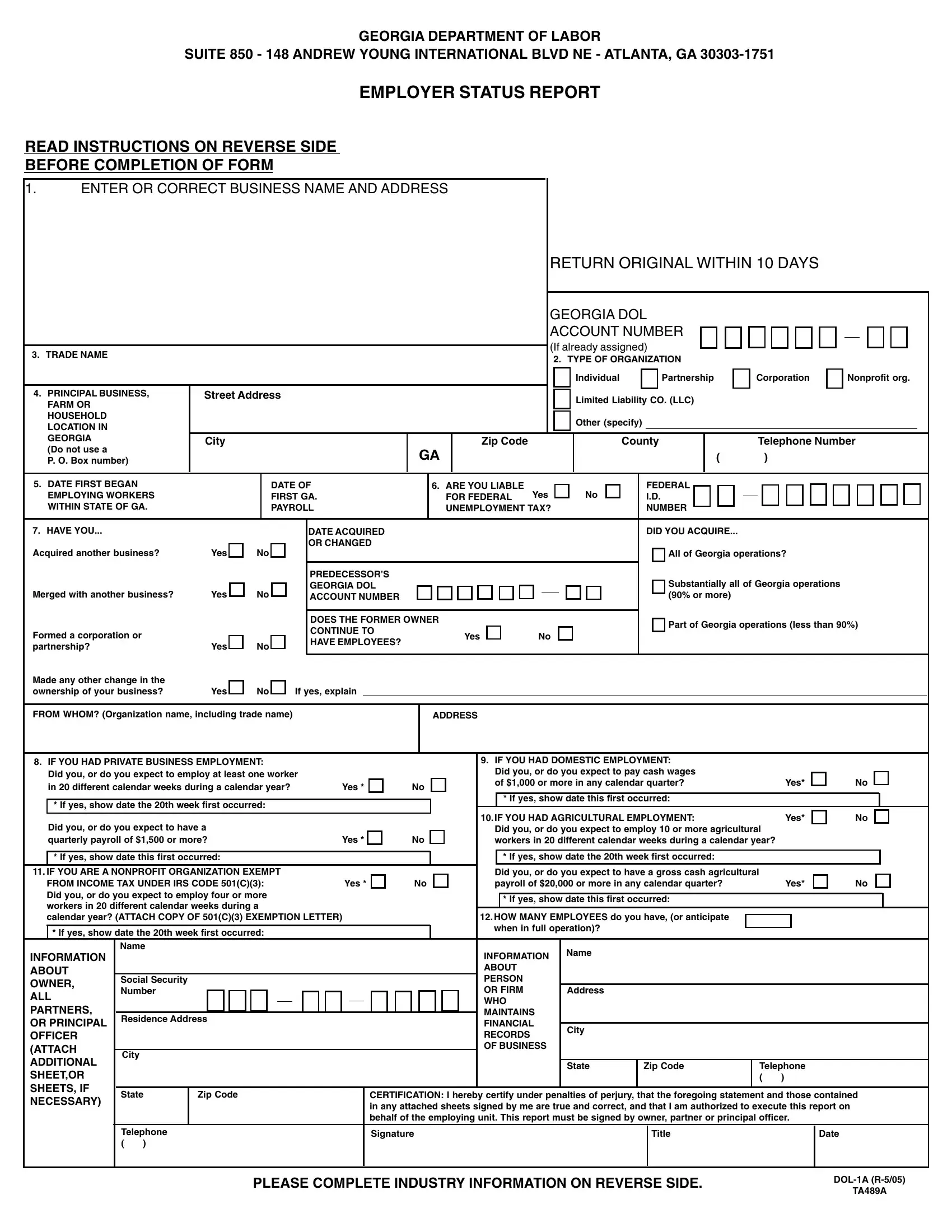
Initiating a business in Georgia involves various steps, among which a significant early task is completing the Department of Labor 1A Form, commonly known as the Employer Status Report. This critical form serves multiple functions: it helps determine an employer's liability for federal unemployment tax, facilitates the assignment of a Georgia Department of Labor Account Number, and gathers specific information about the business, including but not limited to the type of organization (e.g., individual, partnership, corporation), trade name, primary business location, and the nature of the business activities. Additionally, the form addresses various employment situations, querying whether the employer has engaged in private, agricultural, domestic employment, or operates as a nonprofit organization. This comprehensive approach not only aids in classifying the business for state labor records but also in ensuring compliance with state law regarding employment and payroll. Employers are prompted to provide detailed information about their operation, including the date they began employing workers in Georgia, if and when they acquired another business, and projections on employee numbers. The nuanced details requested underscore the form's importance in establishing a new or acquired business's legal and operational framework within the state.
| Question | Answer |
|---|---|
| Form Name | Dol 1A Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | SHEETOR, DOL-1, exempting, R-5 |
