
You can fill in ls 1 form dept of labor effortlessly by using our PDFinity® online tool. To retain our editor on the leading edge of practicality, we aim to adopt user-oriented capabilities and improvements on a regular basis. We are always pleased to get feedback - play a vital part in reshaping the way you work with PDF files. Getting underway is easy! All that you should do is adhere to these easy steps below:
Step 1: Access the PDF form in our editor by clicking on the "Get Form Button" at the top of this webpage.
Step 2: Using our advanced PDF editing tool, you are able to accomplish more than simply fill out blank fields. Try all of the features and make your forms seem perfect with custom text incorporated, or fine-tune the original content to perfection - all backed up by an ability to insert any kind of photos and sign the document off.
Be mindful while completing this document. Make certain all necessary blanks are completed properly.
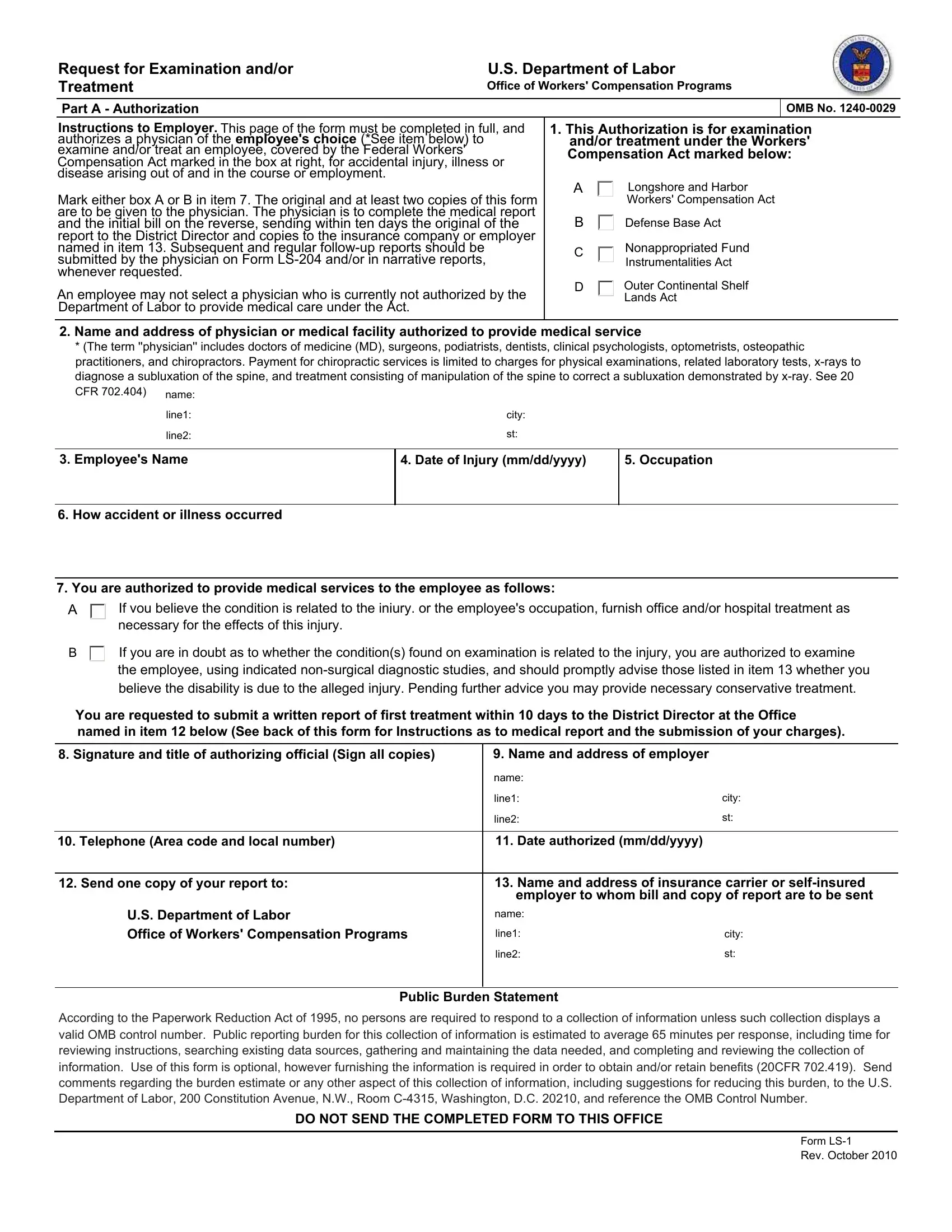
1. To start with, once filling out the ls 1 form dept of labor, start with the page that has the next blanks:
2. After this array of fields is done, you'll want to insert the required details in If vou believe the condition is, If you are in doubt as to whether, You are requested to submit a, Signature and title of, Name and address of employer, name, line, line, city, Telephone Area code and local, Date authorized mmddyyyy, Send one copy of your report to, Name and address of insurance, employer to whom bill and copy of, and US Department of Labor Office of allowing you to move on to the third stage.
Be very mindful when completing If vou believe the condition is and line, because this is the part where a lot of people make mistakes.
3. Completing Instructions To Physician This, Is there any history or evidence, Yes Please describe, What are your findings include, What is your diagnosis, Do you believe the condition, answer if there is doubt, Yes, a Did injury require, Yes, Complete b c d, Is additional hospitalization, b Name of hospital c Date admitted, d Date discharged, and Surgery If any describe type is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. This specific part arrives with the following fields to fill out: Date of first examination, Dates of treatment, mmddyyyy, Date of discharge from treatment, mmddyyyy, mmddyyyy, Period of disability, if termination date unknown so, Date employee able to resume work, Total disability, Partial disability, From, From, To light work To regular work, and If employee is able to resume.
5. This pdf needs to be concluded within this segment. Here one can find an extensive set of form fields that need correct details for your document submission to be complete: of treatment, Services and supplies must be, or No, Cost, Per, Amount, and Total.

Step 3: Once you've looked again at the information in the fields, click "Done" to conclude your form. Get hold of your ls 1 form dept of labor after you join for a free trial. Quickly view the pdf document from your FormsPal account page, with any modifications and adjustments being conveniently preserved! We don't share or sell the details that you type in when dealing with forms at FormsPal.