The PDF editor was built to be as simple as possible. Since you keep up with the following actions, the process of managing the printable dvir form file will be hassle-free.
Step 1: Find the button "Get Form Here" on the following webpage and press it.
Step 2: You will discover each of the functions which you can use on the template after you've accessed the printable dvir form editing page.
It is essential to provide the following data so you can fill in the file:
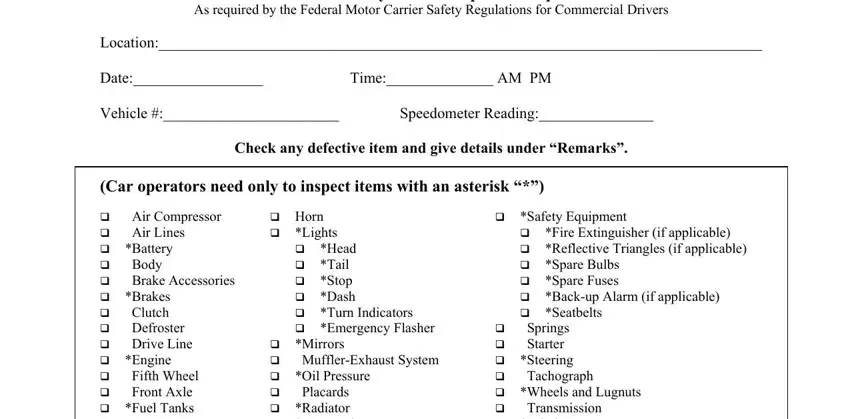
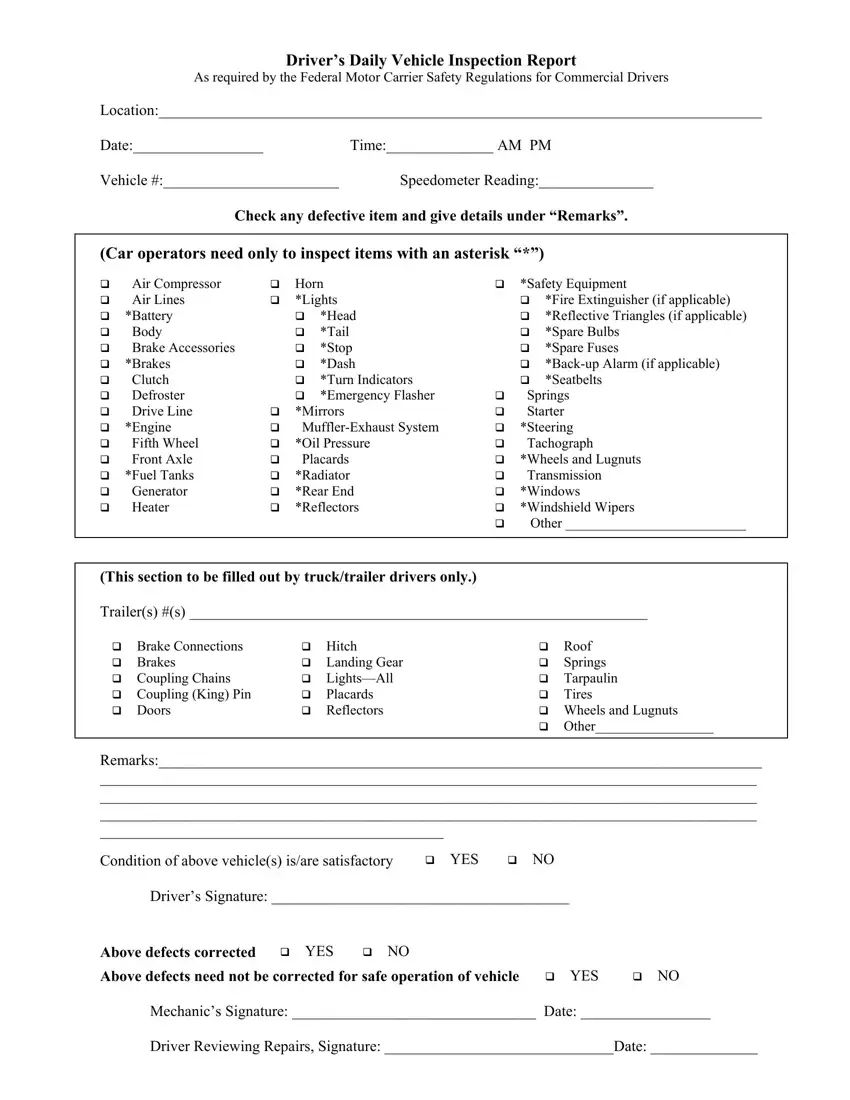
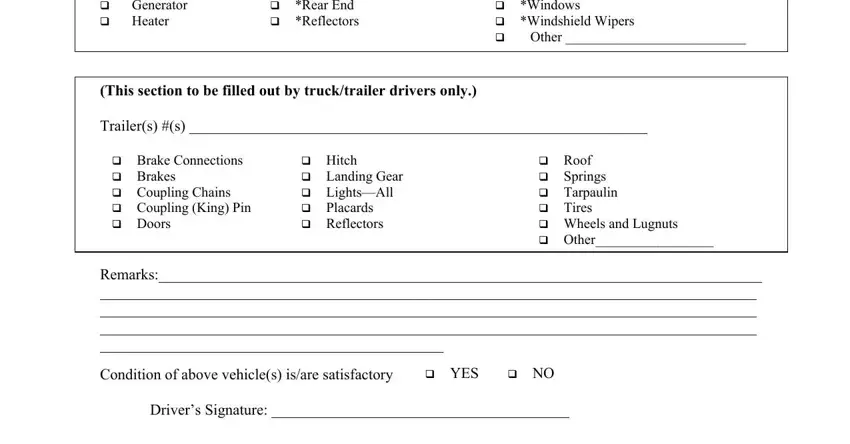
Jot down the information in cid Air Compressor cid Air Lines, cid Mirrors cid MufflerExhaust, cid Springs cid Starter cid, This section to be filled out by, Trailers s, cid Brake Connections cid Brakes, cid Hitch cid Landing Gear cid, cid Roof cid Springs cid Tarpaulin, Remarks, Condition of above vehicles isare, cid YES, cid NO, and Drivers Signature.
The program will request you to give some relevant data to effortlessly fill out the area Above defects corrected, cid YES, cid NO, Above defects need not be, cid YES, cid NO, Mechanics Signature Date, and Driver Reviewing Repairs Signature.
Step 3: Hit the Done button to save the form. So now it is accessible for transfer to your electronic device.
Step 4: In order to avoid probable upcoming difficulties, make sure to get a minimum of two or three copies of every document.
