We found the finest computer programmers to implement the PDF editor. The application will help you complete the disease bwc ohio form simply and won't take too much of your energy. This simple guide will assist you to learn how to start.
Step 1: Choose the button "Get Form Here" on this site and press it.
Step 2: Now, you can change the disease bwc ohio. Our multifunctional toolbar lets you add, get rid of, modify, highlight, and also perform similar commands to the content and areas inside the document.
The next sections are in the PDF file you will be filling in.
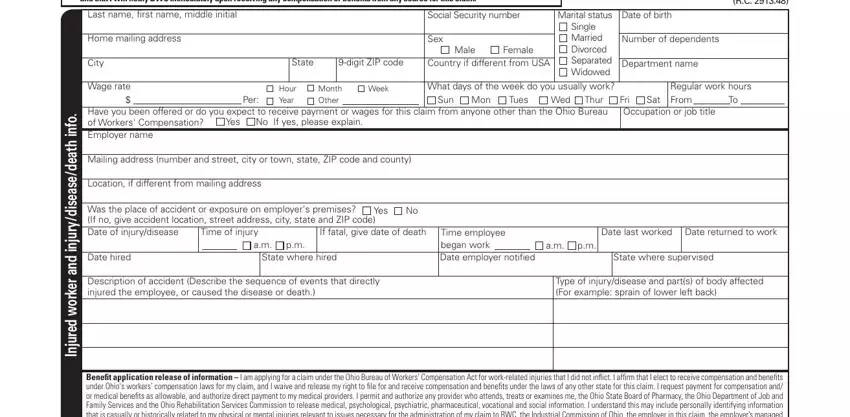
The application will need you to complete the Lastname, rst, name, middle, initial Home, mailing, address City, Wage, rate Social, Security, number Sex, Male, Female, State, digit, ZIP, code Country, if, different, from, USA Dateofbirth, Number, of, dependents Department, name and Per field.
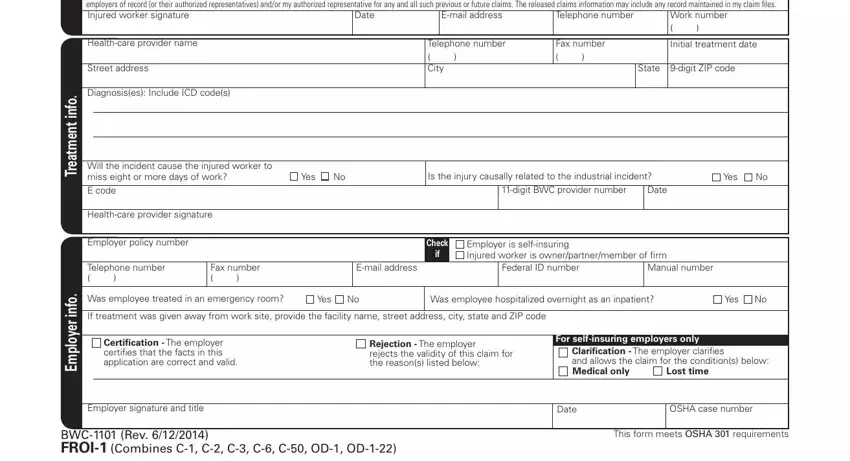
Within the segment discussing Telephone, number Email, address Date, Work, number Healthcare, provider, name Street, address Diagnosis, es, Include, ICD, codes Healthcare, provider, signature Employer, policy, number Telephone, number Fax, number Telephone, number City, Fax, number and Initial, treatment, date one should put down some vital data.
Step 3: As soon as you are done, press the "Done" button to transfer your PDF document.
Step 4: You should make as many duplicates of your document as possible to prevent future problems.
