
You are able to prepare MRA effectively with our PDFinity® PDF editor. The editor is continually maintained by our staff, receiving powerful functions and turning out to be a lot more convenient. To get the process started, go through these simple steps:
Step 1: Press the "Get Form" button above on this page to open our tool.
Step 2: Using our handy PDF tool, it is possible to accomplish more than merely fill in blanks. Try each of the functions and make your forms appear faultless with custom text added, or modify the file's original content to perfection - all that comes with the capability to incorporate any kind of images and sign the document off.
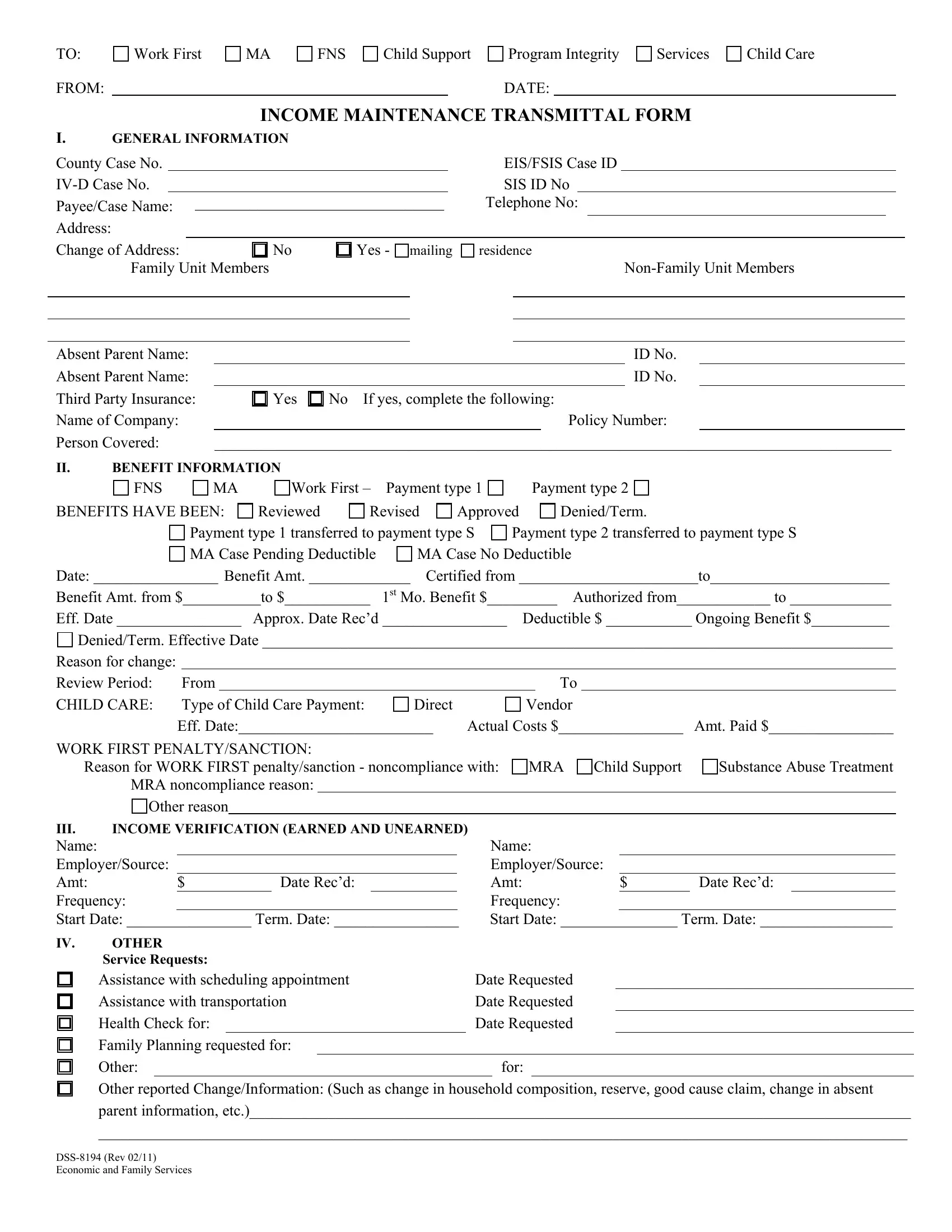
This PDF form will require particular data to be entered, so you must take whatever time to enter what's required:
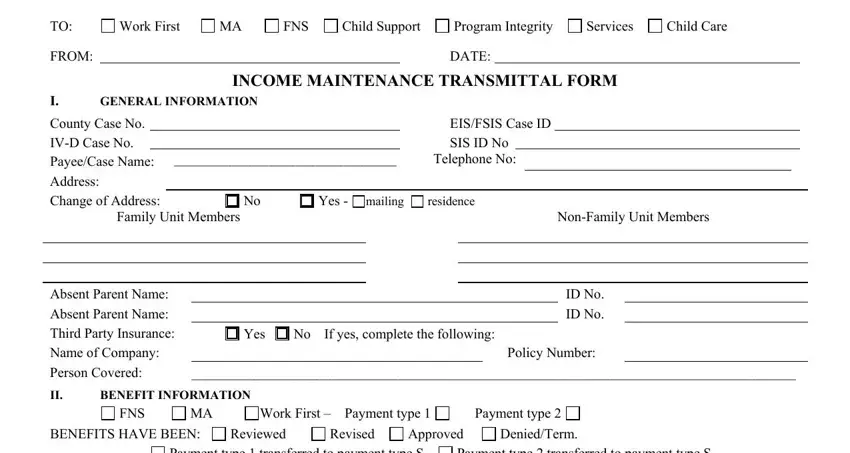
1. While completing the MRA, be certain to complete all of the needed blank fields in its relevant part. This will help hasten the work, allowing your information to be processed fast and accurately.
2. Soon after the prior part is filled out, proceed to enter the applicable information in these: Payment type transferred to, MA Case No Deductible, Payment type transferred to, Date Benefit Amt Certified from, Reason for change Review Period C, From Type of Child Care Payment, Direct, Vendor, Actual Costs Amt Paid, WORK FIRST PENALTYSANCTION, Reason for WORK FIRST, Substance Abuse Treatment, MRA noncompliance reason, Other reason, and INCOME VERIFICATION EARNED AND.
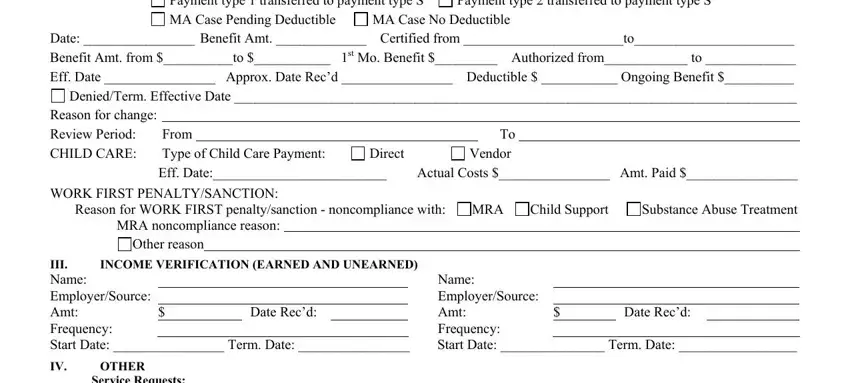
Concerning Direct and Vendor, make sure that you double-check them in this current part. Both of these could be the most significant ones in this file.
3. This next part is all about Service Requests Assistance with, Assistance with transportation, Health Check for, Family Planning requested for, Other, Date Requested, Date Requested, Date Requested, for, Other reported ChangeInformation, and DSS Rev Economic and Family - type in each of these blank fields.
Step 3: Soon after rereading the form fields, hit "Done" and you're done and dusted! Sign up with FormsPal now and instantly obtain MRA, all set for downloading. All alterations you make are preserved , making it possible to modify the file later as needed. FormsPal guarantees your information confidentiality by using a secure method that in no way saves or distributes any type of sensitive information typed in. Be confident knowing your docs are kept confidential whenever you use our editor!