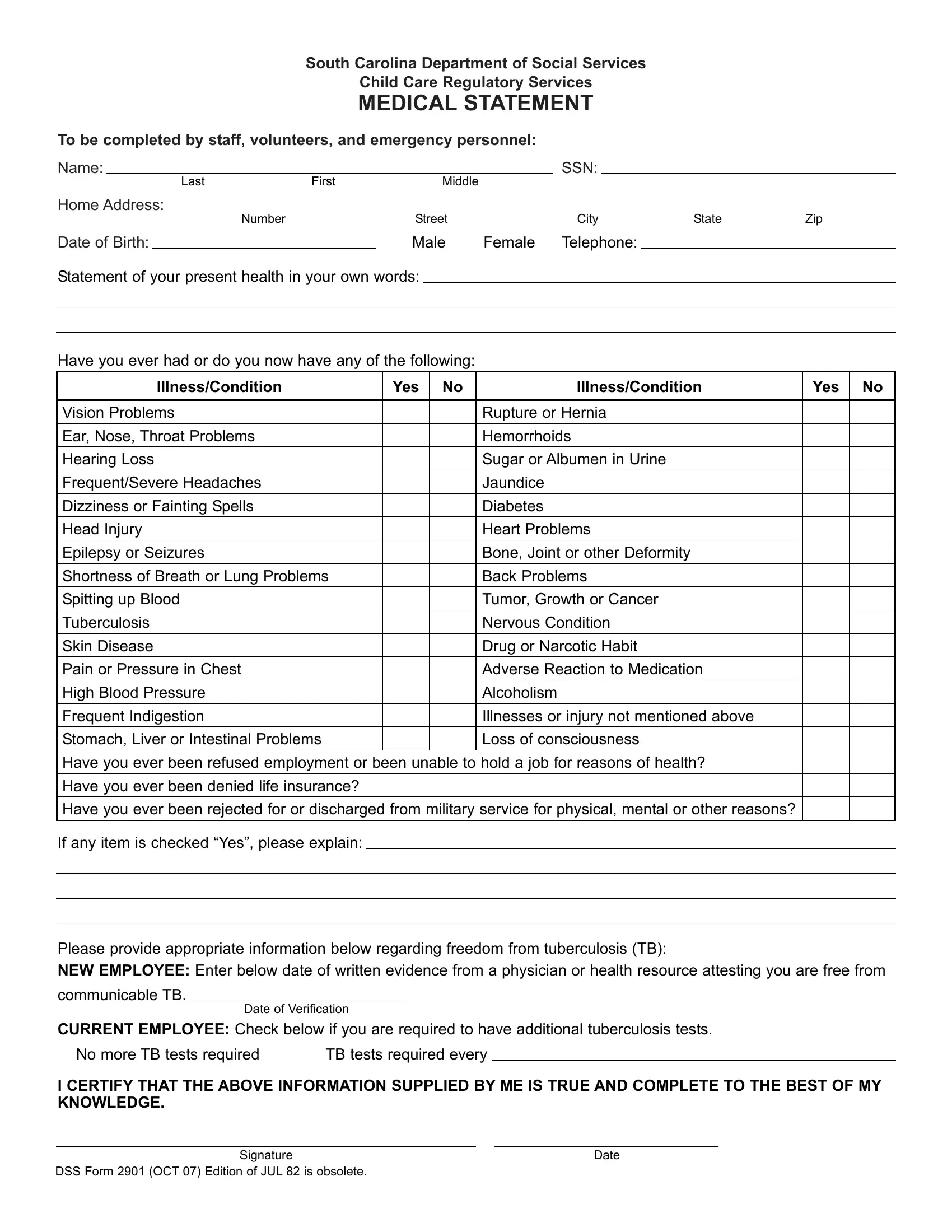
The DSS Form 2901, a pivotal document issued by the South Carolina Department of Social Services Child Care Regulatory Services, is an integral component in ensuring the health and safety of children under care. This comprehensive medical statement is mandatory for staff, volunteers, and emergency personnel engaged in child care services. Its primary aim is to assess the current health status of individuals involved in child care to safeguard against any health-related issues that might compromise the care provided to children. Detailing personal information such as name, social security number, address, and contact details, the form delves into various aspects of an individual's health history. It queries a range of conditions from vision and hearing problems to more severe concerns like heart problems, tuberculosis, and substance abuse, requiring a candid self-assessment of one’s health conditions. Furthermore, the form critically addresses previous instances where one's health might have impacted their employment or insurance opportunities, in addition to military service eligibility. Besides historical health information, it also calls for current tuberculosis (TB) status, distinguishing between new and current employees in terms of TB test requirements. A declaration at the end of the form emphasizes the accuracy and completeness of the provided information, underscoring the form's significance in maintaining a healthy and secure environment for child care services. Thus, the DSS Form 2901 serves as a crucial filter to ensure that those involved in the pivotal role of child care are fit and healthy, ultimately prioritizing the well-being of children in these settings.
| Question | Answer |
|---|---|
| Form Name | Dss Form 2901 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | dss form 2901 medical statement, dss 2901 form, dss form, dss form 2901 sc printable |
South Carolina Department of Social Services
Child Care Regulatory Services
MEDICAL STATEMENT
To be completed by staff, volunteers, and emergency personnel: |
|
|
|
|
|||||
Name: |
|
|
|
|
|
SSN: |
|
|
|
|
|
|
Last |
First |
Middle |
|
|
|
|
Home Address: |
|
|
|
|
|
|
|
||
|
|
|
|
Number |
Street |
City |
State |
Zip |
|
Date of Birth: |
|
|
̈ Male ̈ Female |
Telephone: |
|
|
|||
Statement of your present health in your own words:
Have you ever had or do you now have any of the following:
Illness/Condition |
Yes |
No |
Illness/Condition |
Yes |
No |
|
|
|
|
|
|
Vision Problems |
|
|
Rupture or Hernia |
|
|
|
|
|
|
|
|
Ear, Nose, Throat Problems |
|
|
Hemorrhoids |
|
|
|
|
|
|
|
|
Hearing Loss |
|
|
Sugar or Albumen in Urine |
|
|
|
|
|
|
|
|
Frequent/Severe Headaches |
|
|
Jaundice |
|
|
|
|
|
|
|
|
Dizziness or Fainting Spells |
|
|
Diabetes |
|
|
|
|
|
|
|
|
Head Injury |
|
|
Heart Problems |
|
|
|
|
|
|
|
|
Epilepsy or Seizures |
|
|
Bone, Joint or other Deformity |
|
|
|
|
|
|
|
|
Shortness of Breath or Lung Problems |
|
|
Back Problems |
|
|
|
|
|
|
|
|
Spitting up Blood |
|
|
Tumor, Growth or Cancer |
|
|
|
|
|
|
|
|
Tuberculosis |
|
|
Nervous Condition |
|
|
|
|
|
|
|
|
Skin Disease |
|
|
Drug or Narcotic Habit |
|
|
|
|
|
|
|
|
Pain or Pressure in Chest |
|
|
Adverse Reaction to Medication |
|
|
|
|
|
|
|
|
High Blood Pressure |
|
|
Alcoholism |
|
|
|
|
|
|
|
|
Frequent Indigestion |
|
|
Illnesses or injury not mentioned above |
|
|
|
|
|
|
|
|
Stomach, Liver or Intestinal Problems |
|
|
Loss of consciousness |
|
|
|
|
|
|
|
|
Have you ever been refused employment or been unable to hold a job for reasons of health? |
|
|
|||
|
|
|
|
|
|
Have you ever been denied life insurance? |
|
|
|
|
|
|
|
|
|
|
|
Have you ever been rejected for or discharged from military service for physical, mental or other reasons? |
|
|
|||
If any item is checked “Yes”, please explain:
Please provide appropriate information below regarding freedom from tuberculosis (TB):
NEW EMPLOYEE: Enter below date of written evidence from a physician or health resource attesting you are free from
communicable TB.
Date of Verification
CURRENT EMPLOYEE: Check below if you are required to have additional tuberculosis tests.
̈ No more TB tests required |
̈ TB tests required every |
I CERTIFY THAT THE ABOVE INFORMATION SUPPLIED BY ME IS TRUE AND COMPLETE TO THE BEST OF MY KNOWLEDGE.
Signature |
Date |
DSS Form 2901 (OCT 07) Edition of JUL 82 is obsolete. |
|